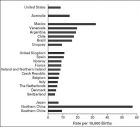
【科普一下脊柱裂脊髓膜膨出的发病率、生存率、致残率、致残原因】 (题目中写肖氏反射弧手术只为好归档和吸引眼球) 请注意:1,死亡原因主要为尿毒症,2,很少病人能活到成年,3,肖氏反射弧手术主要解决这2个问题。 一、发病率:平均约为千分之一新生儿,请注意中国北方接近千分之六新生儿 脊柱裂脊髓膜膨出发病率 【 Botto LD , et al. Neural Tube Defects. N Eng J Med. 341(20):1509-1519,1999 】 二、脊柱裂婴儿的 5 年存活率和致残率 5 年平均大手术 3 次 Althouse R, Wald N. Survival and handicap of infants with spina bifida. Arch Dis Child. 1980 Nov;55(11):845-50. 【摘要】 年 5 年存活率: 37% ( 79/213 新生儿) 存活的79个患儿残废率:52人严重伤残,14人中度伤残。(66/79) 年平均大手术 6 一项随访研究调查了从 1965 年到 1972 年出生于英国牛津郡和伯克希尔西部的 213 名先天性显性脊椎裂(包括 encephalocele and occipital meningocele )患儿。 有脊膜膨出的患儿, 5 年的存活率是 36% ( 107 个婴儿中仅有 39 人存活 5 年以上); 仅有脊柱裂而无脊髓膜膨出的婴儿, 5 年的存活率是 60% ( 50 个婴儿中有 30 人存活 5 年以上);对那些脊髓和脊髓膜几乎都有膨出而不能列入上述两种分类的婴儿, 5 年的存活率只有 18% ( 56 个这样的婴儿仅有 10 人存活 5 年以上)。对那些存活下来的儿童通过 Lorber 标准评估了他们的伤残程度: 存活下来的 49 名脊膜膨出的儿童(包括脊髓脊膜膨出)有 41 人( 84% )属于严重伤残, 4 人( 10% )属于中度伤残,只有 3 人( 6% )是没有伤残;存活下来的 30 名脊柱裂患儿中, 11 人( 37% )属于严重伤残, 10 人( 33 )属于中度伤残,剩下的 9 人( 30% )没有伤残 。 当这种病变发生在头部时(脑膜膨出)更容易导致严重伤残( 75% , 8 名婴儿中有 6 人);仅有脊柱裂患儿的严重伤残率是 23% ( 22 名婴儿中只有 5 人)。 脊膜膨出并存活至少 5 年的患儿,前 5 年平均住院至少 6 个月,并且接受平均至少 6 次大的外科手术 。比较起来, 仅有脊柱裂的患儿(存活至少 5 年),住院的时间少三分之一,平均大手术次数少于 3 次 。在本研究期间对患儿采用现在普遍使用的选择性治疗方案。所有婴儿在出生前均进行产前检查。因此,本研究结果可能有助于评估产前筛检脊髓膜膨出型脊柱裂的意义。 【 Abstract 】: A follow-up study was carried out on 213 infants born with spina bifida cystica (including encephalocele and occipital meningocele) from 1965 to 1972 to women resident in Oxfordshire and the western part of Berkshire. The 5-year survival rate was 36% (39/107) for those with open lesions, 60% (30/50) for those with closed ones, and 18% (10/56) for those with lesions which could not be classified (not known) but which were probably nearly all open. The extent of handicap among these survivors was assessed by means of criteria described by Lorber; among those with open lesions (including 'not known') 84% (41/49) were severely handicapped, 10% (4/49) were moderately handicapped, and only 6% (3/49) had no handicap; among those with closed lesions, 37% (11/30) were severely handicapped, 33% (10/30) were moderately handicapped, and the remaining 30% (9/30) were not handicapped. Closed head lesions (encephalocele or occipital meningocele) were more often associated with severe handicap (6/8; 75%) than were closed spinal lesions (5/22; 23%). The children with open lesions who survived for at least 5 years spent, on average, at least 6 months in hospital during the first 5 years of their life and had, on average, at least 6 major surgical operations. In comparison, those with closed lesions spent one-third less time in hospital, and had fewer than half as many operations. During the period of the study a selective treatment policy was adopted typical of that commonly practised now, and all the infants were born before antenatal screening had been introduced. Our results therefore may be helpful in assessing the benefits to be expected from antenatal screening for open spina bifida. 三、先天性脊柱裂脊膜膨出患者足畸形、行走障碍、皮肤溃疡的原因 【摘自:美国医学专业教科书 http://www.scribd.com/doc/48902221/Spina-bifida 】 脊柱裂都导致不同程度的神经和肌肉骨骼损伤,症状可表现为全身瘫痪,或局部麻木,或轻度功能障碍或无明显功能障碍【 15 】。 脊柱裂发生的解剖学位置决定相应运动神经和感觉神经的功能障碍区域。虽然在童年时代, 隐性闭合不全可能不会被发现,随着年龄增长,身高增长,脊髓向其正常位置( L1-L2 )的上升过程中,原发性发育障碍或继发性肿瘤均可导致脊髓不能上升到 L2 位置,这种情况叫 脊髓栓系综合征:患者可发生足畸形,步态障碍,脊柱侧弯,和括约肌功能障碍 。【脊膜膨出患者一出生基本均有脊髓栓系综合征。一生可能需要多次作栓系松解手术以缓解下肢症状—译者注】 足畸形者,因为骨畸变和足部生物力学的改变,更易产生溃疡 骨畸形能改变处于足底的天然脂肪垫(脂肪垫的作用是把受力均匀地分布在较大区域)。这样,在步行中着地时和足跟抬升期会产生过量的局部压力,可能造成在骨突起部位的皮损或角质增生。 这些足部变化会使得足部溃疡的机会增加两个数量级 。剪切力,压力和摩擦力也都可能有导致骨突起异常区域皮肤破损、溃疡。 溃疡风险与风险因子成正比:外周神经病变患者的溃疡风险高 1.7 倍,同时有外周神经病变和足畸形者风险高 12 倍,同时有外周神经病变加足畸形患者加截肢患者风险高 36 倍 。 【英文原文】 【 http://www.scribd.com/doc/48902221/Spina-bifida 】 Spina bifida is associated with varying degrees of neurologic and musculoskeletal impairment and ranges from complete paralysis and/or paresthesia to minimal or no impairment. The anatomic level of the lesion generally correlates with the motor and sensory deficit. Although the occult dysraphic state may go undetected in early childhood, as the spinal cord ascends to its normal position in life (L1-L2), patients may later present with foot deformities, gait disturbances, scoliosis, and sphincter dysfunction. The failure of the spinal cord to ascend secondary either to primary malformation or to secondary tumor is known as tethering of the cord. Foot deformities make the foot more vulnerable to ulceration via bony deformities and altered foot biomechanics. Bony deformities alter the natural protective fat pads located on the plantar surface of the foot, which normally protect the foot by distributing weight-bearing forces evenly over a large area. Excessive focal pressure developed during the midstance and heel-rise parts of the gait cycle may cause skin loss or hypertrophy of the stratum corneum (callus) over bony prominences. These changes in the foot increase the possibility of ulceration by two orders of magnitude. Shearing, pressure, and frictional forces also all play a role in the breakdown of the cutaneous barrier, since they are concentrated over the abnormal bony prominences. The risk of ulceration is proportional to the number of risk factors and is increased by 1.7 in persons with peripheral neuropathy, by 12 in patients with peripheral neuropathy and foot deformity, and by 36 in those who have peripheral neuropathy, foot deformity, and previous amputation, as compared with those without risk factors.
 标签: 致残率
标签: 致残率