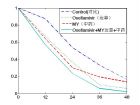
我国中药治疗“甲流”效果获国际认可(附原文) 发布时间: 2011-08-23 | 作者:周婷玉 http://www.stdaily.com 2011年08月23日 ■医卫动态 国际权威医学期刊《内科学年鉴》16日发表我国学者的临床研究结果。这一研究显示,中药汤剂可有效缓解甲型H1N1流感引起的发热症状,其效果与达菲相仿或有更加优效趋势。 记者18日从首都医科大学附属北京朝阳医院——北京呼吸疾病研究所获悉,这一关于奥司他韦(达菲)和传统中药汤剂(麻杏石甘汤和银翘散加减方)治疗甲型H1N1流感(简称甲流)的临床研究是由该所及卫生部北京医院王辰教授领衔、由国内11家医院组成的课题组共同完成。 这一研究在《内科学年鉴》的发表,标志着国际权威医学刊物对我国中医药学研究的认可。研究以科学的方法向世界展示了中医药在人类应对新发呼吸道传染病和突发公共卫生事件中的作用,是中医药研究走向世界进程中具有标识性的重要事件。文章发表后受到国际广泛关注,包括美国卫生部网站在内的3万多个国际主流网站对相关报道进行了转载。 研究采用规范、严格的现代循证医学研究方法,将410例确诊为轻症甲流的成年患者随机分为4组:对照组、达菲组、中药组(应用麻杏石甘汤和银翘散加减方汤剂)、达菲加中药组。结果发现,对照组的发热持续时间为26小时,达菲组的发热时间为20小时,中药组的发热时间只有16小时,达菲加中药汤剂患者的发热时间为15小时。统计分析显示,三个用药组的发热时间均显著短于对照组,中药汤剂可以显著降低甲流发热持续时间。 因为麻杏石甘汤和银翘散加减方中有炙麻黄,含有麻黄碱成分,而一些国家对含有麻黄碱的药物是禁用的。针对西方学者对麻黄毒副作用的担心,课题组解释,方剂中麻黄的使用剂量很小,完全在中医药典的安全剂量范围内。而且,研究观察的205例使用该方剂的患者中未见较大剂量麻黄所引起的心率加快、血压高等副作用,安全性好。 据介绍,2009年秋天,为应对甲流疫情,有关中西医专家提出应当迅速组织评价、验证传统中医药对于甲流的预防与治疗效果,以在达菲储量不足或病毒对达菲出现耐药的情况下提供有效的防治药物。经中西医专家联合讨论,决定采用我国传统上用于“热病”治疗的麻杏石甘汤和银翘散的加减方作为统一处方,所含12味中药均采用同一产地、同一批号的饮片。汤剂制作过程采用严格的标准操作程序,确保中药饮片煎制后其成分固定。经严密筹备,课题组启动了此项在以现代科学方法验证中医药有效性、寻找应对突发呼吸道传染病疫情方面具有极为重要意义的研究。 《内科学年鉴》创刊于1927年,是美国内科医师学院的官方杂志,为世界权威医学杂志,被公认为国际内科学领域“第一刊”。 (新华社) (文·周婷玉) 本篇文章来源于 科技网|www.stdaily.com 原文链接: http://www.stdaily.com/kjrb/content/2011-08/23/content_339704.htm 原文如下( http://www.annals.org/content/155/4/217.full ): Original Research Oseltamivir Compared With the Chinese Traditional Therapy Maxingshigan–Yinqiaosan in the Treatment of H1N1 Influenza A Randomized Trial Chen Wang , MD, PhD ; Bin Cao , MD ; Qing-Quan Liu , MD ; Zhi-Qiang Zou , MD ; Zong-An Liang , MD ; Li Gu , MD ; Jian-Ping Dong , MD ; Li-Rong Liang , MD ; Xing-Wang Li , MD ; Ke Hu , MD ; Xue-Song He , MD ; Yan-Hua Sun , MD ; Yu An , MD ; Ting Yang , MD ; Zhi-Xin Cao , MD ; Yan-Mei Guo , MD ; Xian-Min Wen , MD ; Yu-Guang Wang , MD ; Ya-Ling Liu , MD ; and Liang-Duo Jiang , MD + Author Affiliations From Beijing Chao-Yang Hospital, Beijing Institute of Respiratory Medicine, Capital Medical University, and Beijing Hospital, Ministry of Health, Beijing; Dongzhimen Hospital Affiliated to Beijing University of Chinese Medicine, Beijing; Yantai Infectious Disease Hospital, Shandong; Chengdu Infectious Disease Hospital, Sichuan; Beijing Haidian Hospital, Beijing; Beijing Ditan Hospital, Institute of Infectious Diseases, Capital Medical University, Beijing; Renmin Hospital of Wuhan University; Changxindian Hospital of Fengtai District of Beijing, Beijing; Second Hospital of Chaoyang District of Beijing, Beijing; Second Hospital of Beijing, Beijing; and West China Medical School, West China Hospital, Sichuan University, Sichuan, China. Next Section Abstract Background: Observational studies from Asia suggest that maxingshigan–yinqiaosan may be effective in the treatment of acute H1N1 influenza. Objective: To compare the efficacy and safety of oseltamivir and maxingshigan–yinqiaosan in treating uncomplicated H1N1 influenza. Design: Prospective, nonblinded, randomized, controlled trial. (ClinicalTrials.gov registration number: NCT00935194 ) Setting: Eleven hospitals from 4 provinces in China. Patients: 410 young adults aged 15 to 59 years with laboratory-confirmed H1N1 influenza. Intervention: Oseltamivir, 75 mg twice daily; maxingshigan–yinqiaosan decoction (composed of 12 Chinese herbal medicines, including honey-fried Herba Ephedrae), 200 mL 4 times daily; oseltamivir plus maxingshigan–yinqiaosan; or no intervention (control). Interventions and control were given for 5 days. Measurements: Primary outcome was time to fever resolution. Secondary outcomes included symptom scores and viral shedding determined by using real-time reverse transcriptase polymerase chain reaction. Results: Significant reductions in the estimated median time to fever resolution compared with the control group (26.0 hours ) were seen with oseltamivir (34% ; P 0.001), maxingshigan–yinqiaosan (37% ; P 0.001), and oseltamivir plus maxingshigan–yinqiaosan (47% ; P 0.001). Time to fever resolution was reduced by 19% (CI, 0.3% to 34%; P = 0.05) with oseltamivir plus maxingshigan–yinqiaosan compared with oseltamivir. The interventions and control did not differ in terms of decrease in symptom scores ( P = 0.38). Two patients who received maxingshigan–yinqiaosan reported nausea and vomiting. Limitations: Participants were young and had mild H1N1 influenza virus infection. Missing viral data precluded definitive conclusions about viral shedding. Conclusion: Oseltamivir and maxingshigan–yinqiaosan, alone and in combination, reduced time to fever resolution in patients with H1N1 influenza virus infection. These data suggest that maxingshigan–yinqiaosan may be used as an alternative treatment of H1N1 influenza virus infection. Primary Funding Source: Beijing Science and Technology Project and Beijing Nova Program. Editors' Notes Context Some speculate that the herbal therapy maxingshigan–yinqiaosan could serve as an alternative therapy to antivirals. Contribution In this randomized trial that compared maxingshigan–yinqiaosan with oseltamivir alone, oseltamivir plusmaxingshigan–yinqiaosan, and no treatment in mildly ill patients with confirmed H1N1 influenza, fever resolved sooner in all 3 therapeutic groups than in the group that received no treatment. Caution Ephedra is an ingredient of maxingshigan–yinqiaosan; it is legally unavailable in settings in which ephedra is banned. The study could not determine whether the observed effects of maxingshigan–yinqiaosan were due to antipyretic or antiviral effects. Implication Among patients with mild H1N1 infection, maxingshigan–yinqiaosan speeds fever resolution similarly to oseltamavir. —The Editors In April 2009, cases of human infection with H1N1 influenza A virus were identified in the United States (1) and Mexico (2) and spread rapidly to other regions of the world (3) , resulting in the first influenza pandemic since 1968. As of March 2010, almost all countries had reported cases, and more than 17700 deaths among laboratory-confirmed cases had been reported to the World Health Organization (4) . Influenza A pandemic is typically characterized by abrupt onset of fever, nonproductive cough, sore throat, headache, and myalgia. The illness is usually self-limited, with relief of symptoms within 5 to 7 days (5) . Nevertheless, it is an important disease owing to its ease of communicability and the possibility of severe complications (6, 7) . The antiviral agent oseltamivir was widely used during the H1N1 influenza A pandemic, as recommended by the World Health Organization (8) . Observational studies of hospitalized patients with pandemic H1N1 influenza A infection have suggested that treatment with oseltamivir may reduce severity of and mortality from the disease (9) . However, no direct comparative evidence on the role of oseltamivir in the current novel H1N1 influenza A pandemic has been reported. Isolates of pandemic H1N1 influenza A virus with resistance to oseltamivir have been detected (10) . In resource-limited settings, such as rural areas of China, where the supply of oseltamivir was often insufficient, traditional Chinese medicine (TCM) was used as an alternative therapy. Traditional Chinese medicine has been used to treat seasonal influenza for thousands of years (11) . In a recent meta-analysis of 31 randomized clinical trials including 5514 cases of influenza (12) , the authors concluded that TCM had significantly increased clinical efficacy compared with placebo or no intervention (93.46% vs. 79.03%, respectively; odds ratio, 3.99 ; P 0.001), and no serious adverse effects were reported. Modern pharmacologic studies demonstrated that some TCM formulas had antiviral and immunomodulating effects (13, 14) . During the early days of the 2009 H1N1 influenza A pandemic, the popular herbal formula maxingshigan–yinqiaosan was used widely by TCM practitioners to reduce symptoms. We sought to compare the efficacy and safety of oseltamivir, TCM, and no treatment in adults and adolescents with uncomplicated 2009 H1N1 influenza A virus infection. Persons with mild illness who do not have high-risk conditions do not usually require testing or treatment, and the decision about whether to initiate antiviral therapy is individualized on the basis of the clinician's judgment and on what is known about the benefits of therapy. Therefore, it was ethically possible for us to include a control group that received no intervention. Previous Section Next Section Methods Study Design We conducted a prospective, randomized, controlled, nonblinded, multicenter trial during the H1N1 influenza A epidemic between July and November 2009 at 11 medical sites in 4 provinces in China. The institutional review board of Beijing Chao-Yang Hospital reviewed and approved the protocol and consent forms before the start of the study. All participants signed written informed consent forms before enrollment. Patient Enrollment Patients aged 15 to 70 years who presented within 72 hours of onset of H1N1 influenza A symptoms were enrolled. All patients were admitted to hospitals, where they could be quarantined and observed. Patients who fulfilled all of the following criteria were included: documented body temperature 37.5°C or greater, 1 or more respiratory symptoms (cough, sore throat, or rhinorrhea), and a positive result for H1N1 influenza A virus on real-time reverse transcriptase polymerase chain reaction (RT-PCR). Women were required to have a negative urine pregnancy test before drug administration. Patients were excluded if they had received influenza vaccination in the 12 months before the start of the study; had active, clinically significant chronic illness or HIV disease; were receiving systemic steroids or other immunosuppressants; had taken Chinese medicinal herbs or antivirals; or had new infiltrate of the lungs on chest radiography. Drug Administration The TCM formula that we used in our study was maxingshigan–yinqiaosan, which is composed of 12 herbs: zhimahuang (honey-fried Herba Ephedrae), 6 g; zhimu (Rhizoma Anemarrhenae), 10 g; qinghao (Herba Artemisiae Annuae), 15 g; shigao (Gypsum Fibrosum), 30 g; yinhua (Flos Lonicerae Japonicae), 15 g; huangqin (Radix Scutellariae), 15 g; chaoxingren (stir-baked Semen Armeniacae Amarum), 15 g; lianqiao (Fructus Forsythiae), 15 g; bohe (Fructus Forsythiae), 6 g; zhebeimu (Bulbus Fritillariae Thunbergii), 10 g; niubangzi (Fructus Arctii Tosum), 15 g; and gancao (Radix Et Rhizoma Glycyrrhizae), 10 g. Appendix Table 1 lists the names of these herbs in Chinese and English. View this table: In this window In a new window Appendix Table 1. Chinese Simplified Script and Traditional Script and English Translations of Traditional Chinese Medicines Mentioned in This Article The criteria for the quality of the herbs we used were in accordance with the 2005 Chinese pharmacopoeia (15) . All herbs were distributed to the 11 study sites from the same source. Before the start of the trial, the herbs were tested for heavy metals, microbial contamination, and residual pesticides; all results met safety standards in China. Laboratory personnel were blinded to the identity of the herbs. At each study site, a trained technician prepared the decoction according to a standardized procedure; each unit of formula yielded 800 mL of decoction. Oseltamivir was given as capsules, and the TCM intervention was given as a decoction. Placebo capsules were not used; the control group received no intervention. After agreeing to participate, signing the informed consent form, and completing the baseline visit, all patients were randomly assigned to 1 of the 3 active treatment groups or the control group by using random-number tables with a block size of 8 (SPSS software, version 13.0 ). Randomization was stratified by the 4 study centers, located in Beijing, Yantai, Chengdu, and Wuhan. These centers were selected to ensure broad geographic spread and representation of H1N1 influenza A epidemic areas in mainland China. A statistician who was not involved in data collection or analysis produced the randomization list. A coordinator at each site who was blinded to the participants' characteristics assigned the participants to treatment by telephoning a contact at the study coordinating center in Beijing Chao-Yang hospital. The contact was not involved in the number generation and recruitment process. Participants were then randomly allocated to the control group or one of the intervention groups: oral oseltamivir, 75 mg daily for 5 days; maxingshigan–yinqiaosan decoction, 200 mL orally 4 times daily for 5 days; or oseltamivir plus maxingshigan–yinqiaosan. All participants were hospitalized so that they could be quarantined and closely observed and were followed until discharge. Adherence to therapy was assessed by nurses who were blinded to the study. On the basis of the attending physician's judgment, participants were allowed to use acetaminophen if their body temperature was greater than 39°C. Likewise, the need for antibiotics was determined by the attending physicians. The use of acetaminophen or antibiotics was recorded on the case record form. Assessment During hospitalization, nurses who were blinded to the study used a mercury thermometer to measure participants' body temperature daily at 2 a.m. to 6 a.m., 6 a.m. to 10 a.m., 10 a.m. to 2 p.m., 2 p.m. to 6 p.m., 6 p.m. to 10 p.m., and 10 p.m. to 2 a.m. The presence and severity of influenza symptoms (cough, sore throat, rhinorrhea, headache, and fatigue) and drug-associated side effects were also recorded daily. Symptom scores (0 = absent, 1 = mild, 2 = moderate, and 3 = severe) were recorded and compared with baseline scores until 5 days after treatment in all groups. The primary efficacy end point was time from randomization to fever resolution (body temperature ≤37°C for ≥24 hours). Secondary outcomes were the proportion of patients who became afebrile (body temperature ≤37°C for ≥24 hours); improvement in symptom scores during the study period; side effects associated with the interventions; and incidence of secondary complications of influenza, such as otitis, bronchitis, sinusitis, and pneumonia. Throat swab specimens were collected from all participants and sent to local branches of the Chinese Center for Disease Control and Prevention for H1N1 influenza A RNA testing by using the protocol from the U.S. Centers for Disease Control and Prevention (16) . Serial real-time RT-PCR for viral RNA titers was performed daily from enrollment until discharge. Statistical Analysis We set the sample size to provide adequate power to detect differences of 12 hours or more in time to fever resolution. Clinical analysis of initial cases of 2009 H1N1 influenza in China demonstrated that the median duration of fever was 3 days (interquartile range, 2 to 4 days) (5) . Randomized, controlled studies have shown that oseltamivir reduced duration of illness of patients with influenza by 25% to 32% (17, 18) . On this basis, the difference of at least 12 hours is accepted in the routine clinical practice of treating 2009 H1N1 influenza. Therefore, 100 patients per study group provided 80% power to detect a significant difference of 12 hours or more in time to fever resolution, assuming an SD of 30 and a 2-sided α value of 0.05 for the primary outcome comparisons. All patients who were randomly assigned were included in all efficacy analyses, and patients were analyzed according to their treatment assignment. Means (SDs) or medians (interquartile ranges) were calculated to summarize continuous variables. For categorical variables, the proportion of patients in each category was calculated. One-way analysis of variance, the Kruskal–Wallis rank-sum test, and the chi-square test, as appropriate, were used to compare baseline characteristics among the 4 groups. For analyses of differences in time to fever resolution among 4 treatment groups, an accelerated failure time model (19) was used to estimate median time to fever resolution and percentage change in time to fever resolution, with adjustment for stratified randomization centers and time since onset of illness less than 48 hours versus 48 to 72 hours. The final model was based on the log-normal distribution. Log-logistic and Weibull models were also considered, but the log-normal model fit the best. Interactions between treatment and center and between treatment and time since onset of illness were tested. Changes in viral titer from baseline to day 5 were assessed with a generalized linear mixed model using PROC GLIMMIX in SPSS. Bonferroni adjustment was performed for multiple comparisons of 4 groups. The interaction of time with treatment was also analyzed in the model. Data on time to fever resolution were missing for 1 participant in the control group. For the primary outcome analysis, this participant was considered as a censored observation in the accelerated failure time models. A P value less than 0.05 was considered statistically significant. All analyses were done by using SPSS for Windows, version 13.0, except for analyses of primary outcome and changes in viral titer; these were performed by using SAS software, version 9.1.3 (SAS Institute, Cary, North Carolina). Role of the Funding Source The Beijing Science and Technology Project and the Beijing Nova Program provided funding for the trial. The funding agencies were involved in study design, data collection, data analysis, and manuscript preparation. All authors had full access to the data, participated in data analysis and manuscript development, and gave final approval of the manuscript. Drs. Bin Cao and Chen Wang were involved in the study design and made final decisions on manuscript content. Previous Section Next Section Results Participant Characteristics We recruited 410 participants aged 15 to 69 years from 11 sites. The mean age was 19.0 years (SD, 6.4), and 57.1% of participants were men. Follow-up lasted 12 hours to 16 days (median, 5.0 days). The median time from onset of illness to randomization was 34.5 hours (interquartile range, 18.0 to 48.0 hours) and did not significantly differ among groups. The Figure shows the disposition of the study participants. Of the 410 participants, 102, 103, and 102 were randomly assigned to receive oseltamivir, maxingshigan–yinqiaosan, and combination therapy, respectively. Baseline demographic characteristics, clinical features, and laboratory findings were similar among the 4 groups ( Table 1 ). View larger version: In this page In a new window Download as PowerPoint Slide Figure. Study flow diagram. MY = maxingshigan–yinqiaosan. * These patients were discharged early and declined to return. View this table: In this window In a new window Table 1. Patient Characteristics Use of antibiotics was similar among all groups at baseline (4.9% to 7.8%; P = 0.88) but was much more frequent in the control group after enrollment (34.3% vs. 15.7% in the oseltamivir group, 9.7% in the maxingshigan–yinqiaosan group, and 7.8% in the combination therapy group; P 0.001). First- or second-generation cephalosporins, clindamycin, azithromycin, levofloxacin, and moxifloxacin were the agents chosen by the attending physicians ( Table 2 ). View this table: In this window In a new window Table 2. Use of Acetaminophen and Antibiotics Clinical Outcomes Table 3 shows the effects of the interventions and control on alleviating illness. According to the accelerated failure time model, the estimated median time to fever resolution was significantly reduced in the oseltamivir group (35% ; P 0.001), the maxingshigan–yinqiaosan group (37% ; P 0.001), and the combination therapy group (47% ; P 0.001) compared with the control group (26.0 hours ) ( Appendix Figure 1 ). When the active treatments were compared with one another, however, only the percentage difference in median time to fever resolution with combination therapy versus oseltamivir alone (−19% ) reached borderline statistical significance. Interactions between treatment and center (randomization strata) and between treatment and time since onset of illness were not statistically significant ( P = 0.51 and P = 0.72, respectively). View this table: In this window In a new window Table 3. Accelerated Failure Time Model Estimates for Median Time to Fever Resolution and Difference in Time to Resolution View larger version: In this page In a new window Download as PowerPoint Slide Appendix Figure 1. Fitted curves from accelerated failure time models for median time to fever resolution. MY = maxingshigan–yinqiaosan. The median baseline symptom score was 3 and did not differ among the 4 groups ( Appendix Table 2 ). No difference in any individual symptom, including cough, sore throat, headache, or fatigue, was observed after treatment. View this table: In this window In a new window Appendix Table 2. Change in Symptom Scores During the Study Period Virologic Outcomes Both baseline swab specimens and specimens collected on days 1 to 5 for evaluation of virus shedding were available for 148 participants. Compared with the 262 patients without viral shedding measurements, these 148 patients had lower symptom scores; a lower proportion of cough, headache, and fatigue; lower leukocyte counts; and longer time from onset of illness to randomization. Therefore, the virus shedding results from these 148 patients were not representative of the entire study population ( Appendix Table 3 ). View this table: In this window In a new window Appendix Table 3. Complications and Adverse Events In this subgroup, the median viral titer in throat swabs at enrollment was similar, and a rapid decrease in virus shedding was observed in all 4 groups ( P 0.001) ( Table 4 and Appendix Figure 2 ). Changes in virus shedding from baseline to day 5 did not differ by treatment group ( P = 0.69 for time-by-treatment interaction) ( Appendix Figure 2 ). View this table: In this window In a new window Table 4. Changes in Viral Titer on Real-Time Reverse-Transcriptase Polymerase Chain Reaction View larger version: In this page In a new window Download as PowerPoint Slide Appendix Figure 2. Mean viral titer among 148 participants for whom results were available. MY = maxingshigan–yinqiaosan. Safety Two patients in the maxingshigan–yinqiaosan group had nausea and vomiting. No side effects were observed in the control, oseltamivir, or combination therapy group ( Appendix Table 4 ). No difference in complications after treatment was observed among the 4 groups: 1 case of pulmonary tuberculosis in the control group, 2 cases of pneumonia in the oseltamivir group, 1 case of bronchitis in the maxingshigan–yinqiaosan group, and no complications in the combination therapy group ( Appendix Table 4 ). View this table: In this window In a new window Appendix Table 4. Baseline Characteristics of Patients Without and Those With Viral Titer Measurements Previous Section Next Section Discussion To our knowledge, this is the first registered randomized, controlled trial to investigate the efficacy and safety of oseltamivir, TCM, and no treatment in H1N1 influenza A. We found that resolution of fever was faster with maxingshigan–yinqiaosan than no intervention, but the improvement in symptoms was not significantly more rapid. Compared with active treatments, the reduction in median time to fever resolution between oseltamivir plus maxingshigan–yinqiaosan and oseltamivir (20.0 hours vs. 16.0 hours ) was only 19% (CI, −34% to −0.3%); this reached borderline statistical significance, but the difference was less than the margin of 12 hours. Therefore, with regard to clinical implication, we could not conclude that maxingshigan–yinqiaosan was superior to oseltamivir. We did not find evidence for differences in reductions in viral shedding; however, viral outcomes were available only for a subgroup of patients who had fewer symptoms and longer time from illness onset to randomization. The mechanism of TCM in the treatment of influenza is complex. Zhao and colleagues (21) found that maxingshigan regulated the percentage of T-cell subpopulation in mice exposed to influenza virus A. Investigators also found that maxingshigan had inhibitory effects on influenza virus A by directly killing the virus, interfering with virus adsorption, inhibiting virus proliferation, and protecting the cells from being infected with virus. Except in terms of inhibiting virus proliferation, maxingshigan performed much better than ribavirin (22, 23) . During the outbreak of the severe acute respiratory syndrome in Hong Kong, Poon and associates (24) showed that 2 herbal formulas had immunomodulating effects. In their study of healthy volunteers, they found that the CD4–CD8 ratio of T lymphocytes was significantly increased after participants received Chinese herbal medicine for 14 days (24) . Administration of Chinese herbs may have beneficial immunomodulatory effects for rapid recovery of viral infections. More studies are needed to clarify the mechanisms of TCM. The preparations of maxingshigan–yinqiaosan that we used are those that have been standard for decades, but their safety has not been fully investigated. In our study, 2 of 103 patients (1.9% ) in the maxingshigan–yinqiaosan group experienced nausea and vomiting, and no adverse effects were reported in the oseltamivir and combination therapy groups. The empirical use of certain Chinese medicines in combination with oseltamivir is advocated for the treatment of influenza in Asia, but little is known about the potential for drug interactions in such combinations. A study from Hong Kong showed that TCM preparations may significantly reduce active metabolism of oseltamivir in plasma, most likely owing to suppression of oseltamivir metabolism and possibly enhanced renal clearance (25) . Given the relatively short course of our study and the relatively healthy participants, more evidence on safety of maxingshigan–yinqiaosan is needed before this agent is used widely. In the United States and Canada, marketing of ephedra and ephedrine-containing stimulant combinations for weight loss and bodybuilding is now restricted or illegal because myocardial infarctions, strokes, and deaths associated with these supplements have been reported (26, 27) . The ban on ephedra-containing supplements continues to be controversial. Ephedra is legal in such countries as Germany, Japan, India, and China, where it is widely used. There is general agreement that ephedra treats symptoms of the common cold, allergic rhinitis, and obstructive sleep apnea. In China, Herba Ephedrae is not used for weight loss, bodybuilding, or increased energy. A large follow-up case study found no evidence of severe cardiovascular risk with prescribed ephedrine (28) , and the suspicion of cardiovascular toxicity of ephedrine was mainly based on spontaneous reporting (29–31) . According to a Chinese pharmacopoeia (15) , Herba Ephedrae (mahuang) has a total alkaloid content of 1% by dry weight, and honey-frying (32) decreases the alkaloid content by 0.194%. The safe daily dose of Herba Ephedrae is 2 to 9 g/d. Overdose of Herba Ephedrae causes serious adverse effects. Oseltamivir is a potent and specific influenza neuraminidase inhibitor and inhibits replication of influenza A and B viruses in vitro (33) . However, direct evidence of clinical effectiveness and safety of oseltamivir in treating the 2009 H1N1 influenza A pandemic is limited. Studies in healthy adults with influenza in the United States and Europe showed that early treatment of oseltamivir (usually within 36 hours of onset) could reduce the median duration of illness by 30% (17, 18) . In a recent systematic review and meta-analysis, Jefferson and colleagues concluded that the efficacy of oral oseltamivir, 150 mg/d, against symptomatic laboratory-confirmed influenza was 73% (34) . However, the benefit of oseltamivir was somewhat less than that reported in randomized, controlled trials of its use in seasonal influenza, and in our trial the duration of fever was shortened by 6 hours in the oseltamivir group compared with the control group. In addition, oseltamivir provides no additional benefit in terms of decrease in symptom scores during treatment. This lesser benefit may be due to delayed initiation of treatment with oseltamivir while awaiting results of real-time RT-PCR for H1N1 influenza A virus. In our study, the median time from onset of illness to randomization was 34.5 hours; 23.2% of patients presented 48 to 72 hours after the onset of symptoms. Participants in our study were relatively young and largely had very mild disease. They were admitted to hospitals for quarantine purposes, not because of the severity of the illness. Because disease was mild in these patients, we could not detect a difference in the rate of improvement of symptoms, except fever, in the intervention groups compared with control. Our findings suggest that maxingshigan–yinqiaosan does not act as an antiviral, whereas the benefit of oseltamivir derives entirely from its antiviral activity. The prudent use of antivirals stems from concern that resistance to these agents develops quickly (35) , and we agree that healthy young adults who are not at risk (unlike infants, children, pregnant women, elderly persons, and patients with chronic comorbid conditions) do not need antivirals to treat influenza (8) . In these persons, maxingshigan–yinqiaosan may be used instead of oseltamivir. Our study has limitations. First, it was not a double-blind, placebo-controlled clinical trial. Oseltamivir was given as capsules, and maxingshigan–yinqiaosan was given as a decoction. During the first months of the pandemic, we could not find appropriate placebos for maxingshigan–yinqiaosan that had a similar color and taste (brown and bitter) before the trial began. However, because we included patients who received no treatment as a control group, we were able to prove that the improvement in fever was not due to the placebo effect. In addition, measurements of temperature and virus shedding are objective findings, and the nurses who measured patients' temperature were unaware of study group assignment. Second, the use of acetaminophen and antibiotics was decided by the attending physicians; however, the proportion and extent of use of acetaminophen was similar in the 4 groups at baseline ( Table 2 ). Acetaminophen was used infrequently and probably had no effect on temperature change. More patients in the control group received antibiotics after enrollment. This is similar to many other febrile illnesses, in which physicians respond to persistent temperature elevation by administering antibiotics. Usually, antibiotics are not called for in that situation. Third, both baseline swab and swabs collected on days 1 to 5 for evaluation of virus shedding were available for only 148 participants. Compared with the 262 patients for whom viral shedding measurements were not available, the 148 patients had lower symptom scores, lower leukocyte counts, and a longer interval between onset of illness and randomization, which means that the virus shedding results from the 148 patients were not representative of the overall study population. The lesser extent of disease and longer interval between onset of illness and randomization might explain why changes in virus shedding from baseline to day 5 did not differ by treatment group. In conclusion, in previously healthy young adults and adolescents who presented with uncomplicated 2009 H1N1 influenza A virus infection, therapy with oseltamivir and maxingshigan–yinqiaosan (alone and in combination) was associated with faster resolution of fever. Maxingshigan–yinqiaosan can be used as an alternative treatment of H1N1 influenza A virus infection when oseltamivir is not available. Previous Section Next Section Article and Author Information Note: Drs. C. Wang, B. Cao, Q.Q. Liu, Z.Q. Zou, Z.A. Liang, L. Gu, J.P. Dong, and L.R. Liang contributed equally to this article. Acknowledgment: The authors thank Drs. Jing Zhao, Lai-Ying Fang, Zhi-Tao Tu, Chun Huang, Xiao-Hui Zhai, Xiao-Li Li, Wei Wu, Ran Li, Yi-Qun Guo, Jing-Ya He, Yong Guo, Yu-Dong Yin, Shufan Song, Na Cui, Lu Bai, and Ling-Ling Su, who participated in collection of clinical data, and Drs. Getu Zhaori, Weili Zhang, and Yiqing Song for assistance in careful editing of the manuscript. They also thank Drs. Hua-Xia Chen, Chun-Jiang Zhao, Xiao-Min Yu, Ran Miao, Ying-Mei Liu, and Li-Li Ren, and Mr. Xiang-Yang Ding for technical support. Grant Support: By the Beijing Science and Technology Project (grants Z08050700020801and Z09000700090903) and the Beijing Nova Program (grant 2007A037). Potential Conflicts of Interest: None disclosed. Forms can be viewed at www.acponline.org/authors/icmje/ConflictOfInterestForms.do?msNum=M10-2829 . Reproducible Research Statement: Study protocol and data set: Not available. Statistical code: Available from Dr. B. Cao (e-mail, caobin1999@gmail.com ). Requests for Single Reprints: Bin Cao, MD, Department of Infectious Diseases and Clinical Microbiology, Beijing Chao-Yang Hospital, Beijing Institute of Respiratory Medicine, Capital Medical University, Gongti South Road, No. 8, Beijing, 100020 China (e-mail, caobin1999@gmail.com ), or Chen Wang, MD, Department of Respiratory Medicine, Capital Medical University; Beijing Institute of Respiratory Medicine; Beijing Key Laboratory of Respiratory and Pulmonary Circulation Disorders; Beijing Hospital, Ministry of Health, Beijing, 100020 China (e-mail, cyh-birm@263.net ). Current Author Addresses: Dr. C. Wang: Department of Respiratory Medicine, Capital Medical University; Beijing Institute of Respiratory Medicine; Beijing Key Laboratory of Respiratory and Pulmonary Circulation Disorders; Beijing Hospital, Ministry of Health, Beijing, 100020 China. Drs. B. Cao and Gu: Department of Infectious Diseases and Clinical Microbiology, Beijing Chao-Yang Hospital, Beijing Institute of Respiratory Medicine, Capital Medical University, Gongti South Road, No. 8, Beijing, 100020 China. Drs. Q.Q. Liu and Jiang: Dongzhimen Hospital Affiliated to Beijing University of Chinese Medicine, Hai Yuncang Road, No. 5, Beijing, 100700 China. Drs. Zou and Guo: Yantai Infectious Disease Hospital, Huan Shan Road, No. 62, Yantai, Shandong Province, 341000 China. Dr. Z.A Liang: West China Medical School, West China Hospital, Sichuan University, Wainan Guoxue Road, No. 37, Chengdu, Sichuan Province, 610041 China. Dr. Dong: Beijing Haidian Hospital, Haidian Road, Beijing, 100080 China. Drs. L.R. Liang, Yang, and Z.X. Cao: Beijing Chao-Yang Hospital, Beijing Institute of Respiratory Medicine, Capital Medical University, Gongti South Road, No. 8, Beijing, 100020 China. Drs. Li and Y.G. Wang: Beijing Ditan Hospital, Institute of Infectious Diseases, Capital Medical University, Jingshun East Road, Beijing, 100018 China. Dr. Hu: Renmin Hospital of Wuhan University, Ziyang Road No. 99, Wuhan, Hubei Province, 430060 China. Dr. He: Changxindian Hospital of Fengtai District of Beijing, Beijing, 100072 China. Dr. Sun: Second Hospital of Chaoyang District of Beijing, Jintai Road, No. 13, Beijing, 100026 China. Dr. An: Second Hospital of Beijing, Xi Rongxian Road, No. 9, Beijing, 100031 China. Drs. Wen and Y.L. Liu: Chengdu Infectious Disease Hospital, Jingjusi South Road, Chengdu, Sichuan Province, 610061 China. Author Contributions: Conception and design: C. Wang, B. Cao, Q.Q. Liu, L. Gu, J.P. Dong, Z.X. Cao, L.D. Jiang. Analysis and interpretation of the data: B. Cao, L. Gu, L.R. Liang, X.W. Li. Drafting of the article: B. Cao, L.R. Liang. Critical revision of the article for important intellectual content: C. Wang, B. Cao, Q.Q. Liu. Final approval of the article: C. Wang, B. Cao. Provision of study materials or patients: J.P. Dong, X.W. Li, K. Hu, Y.H. Sun, X.M. Wen, Y.G. Wang, Y.L. Liu. Statistical expertise: L.R. Liang. Obtaining of funding: C. Wang. Administrative, technical, or logistic support: B. Cao, Z.A. Liang, J.P. Dong, X.W. Li. Collection and assembly of data: B. Cao, Z.Q. Zou, Z.A. Liang, L. Gu, J.P. Dong, L.R. Liang, X.W. Li, K. Hu, X.S. He, Y.H. Sun, Y. An, T. Yang, Y.M. Guo, Y.G. Wang. Previous Section References 1. ↵ Centers for Disease Control and Prevention (CDC) Swine influenza A (H1N1) infection in two children—Southern California, March-April 2009. MMWR Morb Mortal Wkly Rep 2009 58 400 2 pmid: 19390508 Centers for Disease Control and Prevention (CDC). Swine influenza A (H1N1) infection in two children—Southern California, March-April 2009. MMWR Morb Mortal Wkly Rep. 2009;58:400-2. Medline 2. ↵ Centers for Disease Control and Prevention (CDC) Outbreak of swine-origin influenza A (H1N1) virus infection—Mexico, March-April 2009. MMWR Morb Mortal Wkly Rep 2009 58 467 70 pmid: 19444150 Centers for Disease Control and Prevention (CDC). Outbreak of swine-origin influenza A (H1N1) virus infection—Mexico, March-April 2009. MMWR Morb Mortal Wkly Rep. 2009;58:467-70. Medline 3. ↵ Centers for Disease Control and Prevention (CDC) Update: infections with a swine-origin influenza A (H1N1) virus—United States and other countries, April 28, 2009. MMWR Morb Mortal Wkly Rep 2009 58 431 3 pmid: 19407737 Centers for Disease Control and Prevention (CDC). Update: infections with a swine-origin influenza A (H1N1) virus—United States and other countries, April 28, 2009. MMWR Morb Mortal Wkly Rep. 2009;58:431-3. Medline 4. ↵ Pandemic (H1N1) 2009—update 94. Geneva: World Health Organization; 1 April 2010. Accessed at www.who.int/csr/don/2010_04_01/en/index.html on 9 April 2010. 5. ↵ Cao B , Li XW , Mao Y , Wang J , Lu HZ , Chen YS et al. National Influenza A Pandemic (H1N1) 2009 Clinical Investigation Group of China Clinical features of the initial cases of 2009 pandemic influenza A (H1N1) virus infection in China. N Engl J Med 2009 361 2507 17 pmid: 20007555 Cao B, Li XW, Mao Y, Wang J, Lu HZ, Chen YS, et al; National Influenza A Pandemic (H1N1) 2009 Clinical Investigation Group of China. Clinical features of the initial cases of 2009 pandemic influenza A (H1N1) virus infection in China. N Engl J Med. 2009;361:2507-17. CrossRef Medline 6. ↵ Jain S , Kamimoto L , Bramley AM , Schmitz AM , Benoit SR , Louie J et al. 2009 Pandemic Influenza A (H1N1) Virus Hospitalizations Investigation Team Hospitalized patients with 2009 H1N1 influenza in the United States, April-June 2009. N Engl J Med 2009 361 1935 44 pmid: 19815859 Jain S, Kamimoto L, Bramley AM, Schmitz AM, Benoit SR, Louie J, et al; 2009 Pandemic Influenza A (H1N1) Virus Hospitalizations Investigation Team. Hospitalized patients with 2009 H1N1 influenza in the United States, April-June 2009. N Engl J Med. 2009;361:1935-44. CrossRef Medline 7. ↵ Domínguez-Cherit G , Lapinsky SE , Macias AE , Pinto R , Espinosa-Perez L , de la Torre A et al. Critically Ill patients with 2009 influenza A(H1N1) in Mexico. JAMA 2009 302 1880 7 pmid: 19822626 Domínguez-Cherit G, Lapinsky SE, Macias AE, Pinto R, Espinosa-Perez L, de la Torre A, et al. Critically Ill patients with 2009 influenza A(H1N1) in Mexico. JAMA. 2009;302:1880-7. Abstract / FREE Full Text 8. ↵ WHO Guidelines for Pharmacological Management of Pandemic Influenza A(H1N1) 2009 Influenza and Other Influenza Viruses. Geneva: World Health Organization; 20 August 2009. Accessed at www.who.int/csr/resources/publications/swineflu/h1n1_guidelines_pharmaceutical_mngt.pdf on 10 June 2011. 9. ↵ Uyeki T Antiviral treatment for patients hospitalized with 2009 pandemic influenza A (H1N1). N Engl J Med 2009 361 110 pmid: 19923564 Uyeki T. Antiviral treatment for patients hospitalized with 2009 pandemic influenza A (H1N1). N Engl J Med. 2009;361:e110. CrossRef Medline 10. ↵ Baz M , Abed Y , Papenburg J , Bouhy X , Hamelin ME , Boivin G Emergence of oseltamivir-resistant pandemic H1N1 virus during prophylaxis . N Engl J Med 2009 361 2296 7 pmid: 19907034 Baz M, Abed Y, Papenburg J, Bouhy X, Hamelin ME, Boivin G. Emergence of oseltamivir-resistant pandemic H1N1 virus during prophylaxis . N Engl J Med. 2009;361:2296-7. CrossRef Medline 11. ↵ Chan K Chinese medicinal materials and their interface with Western medical concepts. J Ethnopharmacol 2005 96 1 18 pmid: 15588645 Chan K. Chinese medicinal materials and their interface with Western medical concepts. J Ethnopharmacol. 2005;96:1-18. CrossRef Medline 12. ↵ Wang J , Cheng SH , Zhang JY A systematic review of chuanhuning for acute respiratory tract infections. Chinese Archives of Traditional Chinese Medicine 2007 25 2200 3 Wang J, Cheng SH, Zhang JY. A systematic review of chuanhuning for acute respiratory tract infections. Chinese Archives of Traditional Chinese Medicine. 2007;25:2200-3. 13. ↵ Chen N , Ren L . Academic Journal of Guang Dong College of Pharmacy 2004 545 6 Chen N, Ren L. . Academic Journal of Guang Dong College of Pharmacy. 2004;545-6. 14. ↵ Huang JM , Chen DP , Yang LP . Journal of Fujian Traditional Chinese Medicine 2003 34 38 9 Huang JM, Chen DP, Yang LP. . Journal of Fujian Traditional Chinese Medicine. 2003;34:38-9. 15. ↵ Chinese Pharmacopoeia Commission . Beijing People's Medical Publishing House 2005 Chinese Pharmacopoeia Commission. . Beijing: People's Medical Publishing House; 2005. 16. ↵ World Health Organization. CDC Protocol of Realtime RTPCR for Influenza A (H1N1). Geneva: World Health Organization; 28 April 2009. Accessed at www.who.int/csr/resources/publications/swineflu/CDCRealtimeRTPCR_SwineH1Assay-2009_20090430.pdf on 10 June 2011. 17. ↵ Nicholson KG , Aoki FY , Osterhaus AD , Trottier S , Carewicz O , Mercier CH et al. Efficacy and safety of oseltamivir in treatment of acute influenza: a randomised controlled trial. Neuraminidase Inhibitor Flu Treatment Investigator Group. Lancet 2000 355 1845 50 pmid: 10866439 Nicholson KG, Aoki FY, Osterhaus AD, Trottier S, Carewicz O, Mercier CH, et al. Efficacy and safety of oseltamivir in treatment of acute influenza: a randomised controlled trial. Neuraminidase Inhibitor Flu Treatment Investigator Group. Lancet. 2000;355:1845-50. CrossRef Medline 18. ↵ Treanor JJ , Hayden FG , Vrooman PS , Barbarash R , Bettis R , Riff D et al. Efficacy and safety of the oral neuraminidase inhibitor oseltamivir in treating acute influenza: a randomized controlled trial. US Oral Neuraminidase Study Group. JAMA 2000 283 1016 24 pmid: 10697061 Treanor JJ, Hayden FG, Vrooman PS, Barbarash R, Bettis R, Riff D, et al. Efficacy and safety of the oral neuraminidase inhibitor oseltamivir in treating acute influenza: a randomized controlled trial. US Oral Neuraminidase Study Group. JAMA. 2000;283:1016-24. Abstract / FREE Full Text 19. ↵ Patel K , Kay R , Rowell L Comparing proportional hazards and accelerated failure time models: an application in influenza. Pharm Stat 2006 5 213 24 pmid: 17080754 Patel K, Kay R, Rowell L. Comparing proportional hazards and accelerated failure time models: an application in influenza. Pharm Stat. 2006;5:213-24. CrossRef Medline 20. Cheng JT Review: drug therapy in Chinese traditional medicine. J Clin Pharmacol 2000 40 445 50 pmid: 10806595 Cheng JT. Review: drug therapy in Chinese traditional medicine. J Clin Pharmacol. 2000;40:445-50. Abstract 21. ↵ Zhao WN , Lu FG , Zhang W , Zhu YW , He YC Effect of maxing shigan decoction and its alteration on mice T-cell subpopulation exposed to influenza virus A. Practical Preventive Medicine 2007 14 178 280 Zhao WN, Lu FG, Zhang W, Zhu YW, He YC. Effect of maxing shigan decoction and its alteration on mice T-cell subpopulation exposed to influenza virus A. Practical Preventive Medicine. 2007;14:178-280. 22. ↵ Guo F , He YC , Xiao ZZ , Wu CR , Zhang W , Li S et al. Study on effect target of maxing shigan decoction on anti-influenza virus A in vitro. Journal of Traditional Chinese Medicine University of Hunan 2008 28 5 9 Guo F, He YC, Xiao ZZ, Wu CR, Zhang W, Li S, et al. Study on effect target of maxing shigan decoction on anti-influenza virus A in vitro. Journal of Traditional Chinese Medicine University of Hunan. 2008;28:5-9. 23. ↵ Zhang W , Lu FG , He YC , Xiao ZZ , Lu XH , Zhu YW et al. Experimental study on effect of maxing shigan decoction on anti-influenza virus A in vitro. Practical Preventive Medicine 2007 14 1351 3 Zhang W, Lu FG, He YC, Xiao ZZ, Lu XH, Zhu YW, et al. Experimental study on effect of maxing shigan decoction on anti-influenza virus A in vitro. Practical Preventive Medicine. 2007;14:1351-3. 24. ↵ Poon PM , Wong CK , Fung KP , Fong CY , Wong EL , Lau JT et al. Immunomodulatory effects of a traditional Chinese medicine with potential antiviral activity: a self-control study. Am J Chin Med 2006 34 13 21 pmid: 16437735 Poon PM, Wong CK, Fung KP, Fong CY, Wong EL, Lau JT, et al. Immunomodulatory effects of a traditional Chinese medicine with potential antiviral activity: a self-control study. Am J Chin Med. 2006;34:13-21. CrossRef Medline 25. ↵ Chow MS , Chang Q , Zuo J Herb-drug interaction involving oseltamivir and Chinese medicine formula . FASEB J 2008 22 Suppl Chow MS, Chang Q, Zuo J. Herb-drug interaction involving oseltamivir and Chinese medicine formula . FASEB J. 2008;22(Suppl):1136.24. 26. ↵ U.S. Food and Drug Administration. Dietary supplements containing ephedrine alkaloids. 22 August 2006. Accessed at www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm152388.htm on 10 June 2011. 27. ↵ Health Canada requests recall of certain products containing ephedra/ephedrine. 6 February 2007. Accessed at www.preventivehealthtoday.com/alerts/hc_ephedra_020109.html on 10 June 2011. 28. ↵ Hallas J , Bjerrum L , Stvring H , Andersen M Use of a prescribed ephedrine/caffeine combination and the risk of serious cardiovascular events: a registry-based case-crossover study. Am J Epidemiol 2008 168 966 73 pmid: 18756018 Hallas J, Bjerrum L, Stvring H, Andersen M. Use of a prescribed ephedrine/caffeine combination and the risk of serious cardiovascular events: a registry-based case-crossover study. Am J Epidemiol. 2008;168:966-73. Abstract / FREE Full Text 29. ↵ Andraws R , Chawla P , Brown DL Cardiovascular effects of ephedra alkaloids: a comprehensive review. Prog Cardiovasc Dis 2005 47 217 25 pmid: 15991150 Andraws R, Chawla P, Brown DL. Cardiovascular effects of ephedra alkaloids: a comprehensive review. Prog Cardiovasc Dis. 2005;47:217-25. CrossRef Medline 30. ↵ Haller CA , Benowitz NL Adverse cardiovascular and central nervous system events associated with dietary supplements containing ephedra alkaloids. N Engl J Med 2000 343 1833 8 pmid: 11117974 Haller CA, Benowitz NL. Adverse cardiovascular and central nervous system events associated with dietary supplements containing ephedra alkaloids. N Engl J Med. 2000;343:1833-8. CrossRef Medline 31. ↵ Soni MG , Carabin IG , Griffiths JC , Burdock GA Safety of ephedra: lessons learned. Toxicol Lett 2004 150 97 110 pmid: 15068827 Soni MG, Carabin IG, Griffiths JC, Burdock GA. Safety of ephedra: lessons learned. Toxicol Lett. 2004;150:97-110. CrossRef Medline 32. ↵ Yan Y , Zhan L , Chen Z , Kang C . West China Journal of Pharmaceutical Sciences 2007 22 559 61 Yan Y, Zhan L, Chen Z, Kang C. . West China Journal of Pharmaceutical Sciences. 2007;22:559-61. 33. ↵ Moscona A Neuraminidase inhibitors for influenza. N Engl J Med 2005 353 1363 73 pmid: 16192481 Moscona A. Neuraminidase inhibitors for influenza. N Engl J Med. 2005;353:1363-73. CrossRef Medline 34. ↵ Jefferson T , Jones M , Doshi P , Del Mar C Neuraminidase inhibitors for preventing and treating influenza in healthy adults: systematic review and meta-analysis. BMJ 2009 339 b5106 pmid: 19995812 Jefferson T, Jones M, Doshi P, Del Mar C. Neuraminidase inhibitors for preventing and treating influenza in healthy adults: systematic review and meta-analysis. BMJ. 2009;339:b5106. Abstract / FREE Full Text 35. ↵ Dharan NJ , Gubareva LV , Meyer JJ , Okomo-Adhiambo M , McClinton RC , Marshall SA et al. Oseltamivir-Resistance Working Group Infections with oseltamivir-resistant influenza A(H1N1) virus in the United States. JAMA 2009 301 1034 41 pmid: 19255110 Dharan NJ, Gubareva LV, Meyer JJ, Okomo-Adhiambo M, McClinton RC, Marshall SA, et al; Oseltamivir-Resistance Working Group. Infections with oseltamivir-resistant influenza A(H1N1) virus in the United States. JAMA. 2009;301:1034-41.
 标签: 中药治疗
标签: 中药治疗