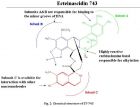
来源于被囊动物红树海鞘 Ecteinascidiaturbinata 的ecteinascidi-743(Et-743,trabectedin)对直肠癌、乳腺癌、肺癌、黑色素瘤等有显著的疗效,2007年10月欧盟已批准该药(商品名Yondelis)用于晚期软组织肿瘤的治疗,成为第一个现代海洋药物。 【药物名称】曲贝替定(Trabectedin), Ecteinascidin 743, NSC-684766, ET-743, Yondelis 【化学名】(1'R,6R,6aR,7R,13S,14S,16R)-5-Acetoxy-6',8,14-trihydroxy-7',9-dimethoxy-4,10,23-trimethyl-1',2',3',4',6a,7,12,13,14,16-decahydro-6H-spiro isoquino benzazocine-20,1'-isoquinolin]-19-one 【CAS登记号】114899-77-3 【结构式】 【分子式】C 39 H 43 N 3 O 11 S 【分子量】761.8447 关于曲贝替定的研究进展以及作用机理请浏览: TRABECTEDIN: A NOVEL MOLECULAR THERAPEUTIC IN CANCER (2013-3-3 15:43:54); A Review of Trabectedin (ET-743): A Unique Mechanism of Action (2013-3-3 15:27:37)
抗血管生成药物被广泛用于癌症治疗。最近,两项分别发表在《Cancer Cell》和《PNAS》杂志的研究揭示,抗血管生成药物会降低其它抗癌药物的效能,增强肿瘤的侵袭性。这两项研究强调,在癌症治疗中要谨慎权衡抗血管生成治疗的利与弊。 《自然》杂志今天发表文章,对这两项研究工作进行了综合评价。 Nature | News Views Cancer: Limitations of therapies exposed Oriol Casanovas Nature Volume: 484 , Pages: 44–46 Date published: (05 April 2012) Published online 04 April 2012 Certain drugs that are used to treat cancer affect blood-vessel formation in tumours. But it seems that these antiangiogenic drugs can reduce the efficiency of other anticancer agents and increase the tumours' aggressiveness. Tumour growth depends on angiogenesis, the formation of new blood vessels, to ensure a continuous supply of oxygen and nutrients. That is why antiangiogenic agents are used to treat certain cancers, either alone or in combination with traditional cytotoxic drugs. However, the mechanistic details of how these combination therapies work are far from clear, and accumulating evidence is exposing their limitations. Writing in Cancer Cell , Van der Veldt et al . 1 report that angiogenesis inhibitors can decrease the delivery of cytotoxic drugs to tumours in patients, and hence hinder the drugs' therapeutic benefits. And in a paper published in Proceedings of the National Academy of Sciences , Conley et al . 2 find that tumours can adapt to antiangiogenic therapy by accumulating particularly aggressive cells. The main target of current antiangiogenic agents is a protein called vascular endothelial growth factor (VEGF), which has a central role in angiogenesis. Although it has been known for several years that VEGF inhibitors provide additional antitumour effects when combined with cytotoxic drugs ( Fig. 1a ), the underlying mechanism has been a mystery since the early positive results of drug-combination trials 3 . The most widespread explanation for such a mechanism, the 'vascular normalization' theory, was proposed in 2001. According to this theory 4 , 5 , antiangiogenic therapy induces structural and functional changes in tumour blood vessels — which have abnormal features — to make them more similar to normal vessels and, as a result, blood flow is increased and cytotoxic drugs can more easily enter the tumour. Figure 1: Drawbacks of anticancer therapies. a , Certain cancers are treated with antiangiogenic drugs (which affect blood-vessel formation), either alone or in combination with cytotoxic agents that inhibit the growth of cancer cells. Some of these cells (green) are particularly dangerous because they can be more resistant to cytotoxic therapy than the other tumour cells and can spread to other organs to seed new tumours. b,c , A decreased blood supply to the tumour, which is the main benefit from antiangiogenic therapy, is also the basis for the therapy's limitations. b , It can reduce the distribution of cytotoxic agents in the tumour, and hence their efficacy. Van der Veldt et al . 1 report one such undesirable outcome in patients with non-small-cell lung cancer. c , By reducing oxygen levels in the tumour, antiangiogenic drugs can induce the accumulation of more aggressive cells that have an increased capacity to spread to other organs. Conley et al . 2 document this phenomenon in mouse models of breast cancer in the absence of a cytotoxic agent. To test the theory in a clinical setting, Van der Veldt and colleagues 1 studied the uptake and retention of a cytotoxic drug (docetaxel) in 10 patients with advanced-stage non-small-cell lung cancer (NSCLC). By using radiolabelled docetaxel together with a sensitive imaging method (positron emission tomography), the authors demonstrate that VEGF inhibition with a drug called bevacizumab induces a fast and sustained decrease — not increase — in the penetration of both water and docetaxel in the tumours ( Fig. 1b ). These results contrast with those of previous studies in patients with rectal cancer 6 and in patients with glioblastoma (a brain tumour) 7 , which showed that bevacizumab treatment induces vascular normalization and increased glucose uptake in the tumours. However, glucose uptake by tumour cells does not, in my opinion, necessarily correlate with cytotoxic-drug delivery and penetration into tumours. The discrepancies between the authors' observations 1 and previous results 6 , 7 could also be due to differences in blood-vessel networks and in the response to angiogenesis inhibitors between the three cancer types, as it is known that these agents can affect blood vessels in different ways in different tissues 7 , 8 . In any case, the finding 1 that, at least in patients with NSCLC, antiangiogenic therapy does not improve cytotoxic drug delivery to tumours — but rather has the opposite effect — exposes a perturbing drawback to such treatments. Indeed, this could be the cause of the modest benefits of these combination therapies in NSCLC and other tumour types 9 . Such a potential shortcoming could be circumvented by optimizing the scheduling of the therapeutic agents. For example, rather than administering both types of drug to a patient during the same period, treatment with blood-distributed cytotoxic agents could be followed by antiangiogenic therapy. Other limitations of the use of angiogenesis inhibitors derive from the fact that tumours are highly adaptable. Although their ability to become resistant to cytotoxic drugs and radiation — another common anticancer therapy — has long been known, it was initially postulated 10 that antiangiogenic drugs would not suffer from the same problem because they target blood vessels rather than tumour cells. Yet preclinical and clinical evidence 11 , 12 has revealed that tumours can indeed adapt and become resistant to antiangiogenic therapy. As if that was not bad enough, angiogenesis inhibitors have been shown 13 , 14 to make some tumours more aggressive in animal models ( Fig. 1c ). To explore this issue, Conley and co-workers 2 implanted human cancer cells (derived from established breast- cancer cell lines) in mice. They then treated the animals with the antiangiogenic agents sunitinib — which inhibits VEGF's main cell-surface receptors — and bevacizumab. The treatment induced an accumulation of certain cancer cells that expressed the enzyme aldehyde dehydrogenase and that, like cancer progenitor cells, could initiate tumours when reimplanted in other mice. Similar cell populations have been described in tissue samples from patients with inflammatory breast cancer 15 and in glioblastoma in mice given combination therapies 16 . Conley et al . 2 go on to delineate a possible cellular and molecular mechanism for the increased aggressiveness and spread capacity of tumours treated with antiangiogenic drugs. They find that the drugs, by inducing oxygen deficiency (hypoxia) in the tumours, activate not only a hypoxia-response program but also the Akt/β-catenin signalling pathway, which regulates cell growth and adhesion between cells. This pathway has been previously implicated in the regulation of breast-cancer progenitor cells 17 . The authors suggest that the drug-induced hypoxia response activates the Akt/β-catenin pathway, which in turn stimulates the growth of specific, more aggressive, cancer-cell populations. How could this drawback of antiangiogenic therapies be overcome? One possibility would be to combine angiogenesis inhibitors with drugs that suppress the cancer cells' response to hypoxia, or with inhibitors of the Akt/β-catenin pathway. Another alternative could be the use of molecules such as modified semaphorin proteins 18 , which can exert dual (or multiple) anticancer effects by simultaneously targeting angiogenesis and blocking tumour spread. Overall, the papers by Van der Veldt et al . 1 and Conley et al . 2 emphasize the need for a carefully balanced evaluation of the benefits and limitations of antiangiogenic therapies. As mentioned above, such treatments could be improved by sequential scheduling of cytotoxic and antiangiogenic drugs, or by smarter combinations of these drugs with others targeting progenitor-cell pathways. In any case, despite many open questions, there is hope that an understanding of the therapies' weaknesses will translate into therapeutic gains. References Van der Veldt, A. A. M. et al . Cancer Cell 21 , 82 – 91 ( 2012 ). CAS PubMed Article Show context Conley, S. J. et al . Proc. Natl Acad. Sci. USA 109 , 2784 – 2789 ( 2012 ). PubMed Article Show context Hurwitz, H. I. et al . J. Clin. Oncol. 23 , 3502 – 3508 ( 2005 ). CAS ISI PubMed Article Show context Jain, R. K. Nature Med. 7 , 987 – 989 ( 2001 ). Article Show context Jain, R. K. Science 307 , 58 – 62 ( 2005 ). CAS ISI PubMed Article Show context Willett, C. G. et al . Nature Med. 10 , 145 – 147 ( 2004 ). Article Show context Batchelor, T. T. et al . Cancer Cell 11 , 83 – 95 ( 2007 ). CAS ISI PubMed Article Show context Kamba, T. et al . Am. J. Physiol. Heart Circ. Physiol. 290 , H560 – H576 ( 2006 ). CAS ISI PubMed Article Show context Sandler, A. et al . N. Engl. J. Med. 355 , 2542 – 2550 ( 2006 ). CAS ISI PubMed Article Show context Boehm, T. , Folkman, J. , Browder, T. O'Reilly, M. S. Nature 390 , 404 – 407 ( 1997 ). CAS ISI PubMed Article Show context Bergers, G. Hanahan, D. Nature Rev. Cancer 8 , 592 – 603 ( 2008 ). Article Show context Rini, B. I. Atkins, M. B. Lancet Oncol. 10 , 992 – 1000 ( 2009 ). CAS ISI PubMed Article Show context Pàez-Ribes, M. et al . Cancer Cell 15 , 220 – 231 ( 2009 ). CAS ISI PubMed Article Show context Ebos, J. M. L. et al . Cancer Cell 15 , 232 – 239 ( 2009 ). CAS ISI PubMed Article Show context Charafe-Jauffret, E. et al . Clin. Cancer Res. 16 , 45 – 55 ( 2010 ). CAS ISI PubMed Article Show context Folkins, C. et al . Cancer Res. 67 , 3560 – 3564 ( 2007 ). CAS ISI PubMed Article Show context Korkaya, H. et al . PLoS Biol. 7 , e1000121 ( 2009 ). CAS PubMed Article Show context Casazza, A. et al . EMBO Mol. Med. 4 , 234 – 250 ( 2012 ). CAS PubMed Article Show context http://www.nature.com/nature/journal/v484/n7392/full/484044a.html#/references
 标签: 抗癌药物
标签: 抗癌药物