博文
[转载]治疗 SMA 罕见病的孤儿药 Onasemnogene Abeparvovec (Zolgensma ® ) 的真实世界
|||
治疗 SMA 罕见病的孤儿药 Onasemnogene Abeparvovec (Zolgensma ® ) 的真实世界安全性数据:基于 EMA 不良事件报告系统的药物警戒研究
Abstract 摘要
The recent introduction of the innovative therapy, onasemnogene abeparvovec (Zolgensma®), has revolutionized the spinal muscular atrophy (SMA) therapeutic landscape. Although Zolgensma® therapy has proven to lead to functional improvements in SMA children, some gaps in its safety profile still need to be investigated. To better characterize the Zolgensma® safety profile, we conducted a retrospective observational study, analyzing all the Individual Case Safety Reports (ICSRs) referred to it and collected in the European pharmacovigilance database between 1 January 2019 and 22 September 2023. We found 661 ICSRs related to Zolgensma®, with a growing trend in the annual reporting. The majority of the reports were sent by healthcare professionals and referred to infant females. In more than 90% of the cases, Zolgensma® was the only reported suspected drug. Out of a total of 2744 reported ADRs, increased hepatic enzymes, pyrexia, vomiting, and thrombocytopenia were the most commonly reported adverse reactions. Of these adverse reactions (ADRs), 56.9% were serious, causing or prolonging the patient’s hospitalization. A total of 39 ICSRs related to cases with a fatal outcome. Alterations in the heart rhythm, acute hepatic failure, and hepatic cytolysis emerged among the cardiac and hepatic disorders, respectively.
最近推出的创新疗法onasemnogene abeparvovec(Zolgensma ® )彻底改变了脊髓性肌萎缩症(SMA)的治疗格局。尽管 Zolgensma ® 疗法已被证明能改善 SMA 儿童的功能,但其安全性方面仍有一些不足之处有待研究。为了更好地描述Zolgensma ® 的安全性特征,我们开展了一项回顾性观察研究,分析了2019年1月1日至2023年9月22日期间欧洲药物警戒数据库中收集的所有与之相关的单个病例安全性报告(ICSR)。我们发现了 661 份与佐尔根斯玛 ® 相关的 ICSR,年度报告呈增长趋势。大多数报告由医疗保健专业人员提交,涉及女婴。在超过 90% 的案例中,佐尔根斯玛 ® 是唯一报告的可疑药物。在总共 2744 例不良反应报告中,肝酶升高、发热、呕吐和血小板减少是最常见的不良反应。在这些不良反应中,56.9%为严重不良反应,导致或延长了患者的住院时间。共有 39 例 ICSR 涉及致命病例。在心脏和肝脏疾病中,分别出现了心律改变、急性肝功能衰竭和肝细胞溶解。
1. Introduction
脊髓性肌萎缩症(SMA)是婴儿死亡的主要遗传原因[ 1]。它是一种罕见的神经肌肉疾病,估计发病率约为每 1 万名活产婴儿中 1 例,发病率为每 10 万人中 1-2 例[2]。肌肉无力和萎缩是 SMA 的典型症状,尤其影响下肢和呼吸肌。在最严重的情况下,这种症状会演变成活动、吞咽和呼吸能力减弱或丧失[3]。脊髓中的α-运动神经元进行性变性和神经肌肉接头发育缺陷是SMA的特征,其原因是存活运动神经元(SMN)蛋白表达减少或缺乏[4]。这种无处不在的蛋白质对运动系统和运动神经元的功能至关重要[1]。SMN由位于染色体5q13上的两个基因编码:端粒SMN1和中心粒SMN2[4]。SMA的遗传原因已被确定为SMN1基因的缺失或突变,而SMN1是唯一能编码全功能SMN蛋白的基因。SMN2 基因主要产生一种功能减弱的 SMN 蛋白,即 SMNΔ7。这种截短的异构体占 SMN2 产物的 85-90%,极不稳定,更容易被泛素-蛋白酶体途径降解。只有 10-15% 的 SMN2 编码产物是功能性蛋白质。SMA的发病年龄和临床病程的严重程度与SMN2拷贝数成反比[5]。根据这三个相关变量,SMA 可分为五种类型,从出生前发病的致命型(0 型)到成年后发病的较轻型(IV 型)。然而,即使在同一类型中,病情也有轻重之分,多达 25% 的患者无法准确分类[6]。婴儿型(I 型 SMA)最为常见,约占患者总数的一半。I 型 SMA 患儿在出生后 6 个月内会出现以下症状:肌张力低下、运动发育迟缓、喂养困难、无法独立坐起[7]。此外,患有 I 型 SMA 的婴儿通常在出生后 2 岁前出现呼吸衰竭,需要长期通气和营养支持[6]。关于治疗的可能性,在 2016 年之前,治疗只能支持生命功能。通过鉴定 SMA 发病和发展的分子机制,我们可以确定一些依赖或不依赖 SMN 的治疗策略。迄今为止,已有三种 SMA 治疗方法,它们都旨在以不同方式提高 SMN 蛋白水平[8]。 特别是,反义寡核苷酸 nusinersen(Spinraza ® )和 risdiplam(Evrysdi ® )都是通过改变 SMN2 的剪接而起作用,而 onasemnogene abeparvovec(Zolgensma ® )则是通过替换 SMN1 基因而起作用
Zolgensma ® 是美国食品药品管理局(FDA)和欧洲医药管理局(EMA)分别于 2017 年和 2020 年批准的首个 SMA 基因疗法[ 9]。这一创新疗法的推出彻底改变了 SMA 的治疗格局[ 10]。迄今为止,Zolgensma ® 适用于治疗 SMN1 基因双等位基因突变且临床诊断为 SMA 1 型的 5q SMA 患者,或 SMN1 基因双等位基因突变且 SMN2 基因多达三个拷贝的 5q SMA 患者[9]。所使用的 AAV9 载体可将 SMN1 基因的功能拷贝传递到运动神经元核,作为功能性 SMN 的主要来源。除了创新的作用机制外,佐尔根斯玛 ® 的最大创新还在于其给药方法,即在 60 分钟内进行一次静脉输注。
这种一次性终生基因替代疗法直接作用于 SMA 的单基因病因[11]。与需要鞘内注射的药物替代品奴西那生(nusinersen)和需要每天口服的药物替代品利地普仑(risdiplam)相比,这一特点意味着向前迈进了一大步。尽管佐尔根斯玛 ® 已被证实能改善接受治疗的 SMA 患儿的功能,减少肺部和营养支持需求以及住院率,并改善运动功能[12],但其安全性方面的一些缺陷仍有待研究[9, 10]。目前仍有一些悬而未决的问题需要解决:其长期益处仍有待确定,批准前的安全性数据需要在真实世界环境中进行确认/拒绝。此外,其心脏毒性、背根神经节毒性和染色体整合导致的致瘤性也是需要调查的重要潜在风险
在这种情况下,上市后数据分析作为尚未出现的新信息来源尤为重要,特别是在特定人群中[14]。有鉴于此,本研究的目的是通过分析从欧洲药物警戒数据库 Eudravigilance (EV) 中检索到的数据,对佐尔甘玛 ® 上市后的安全性进行评估。
2. Results
在我们的研究期间,共向 EV 收集了 661 份与使用 onasemnogene abeparvovec 相关的 ICSR,描述了 2744 个疑似不良反应(ADR)。如图 1 所示,从 2019 年开始,ICSR 报告持续增加,2022 年达到峰值,发送了 209 份 ICSR。
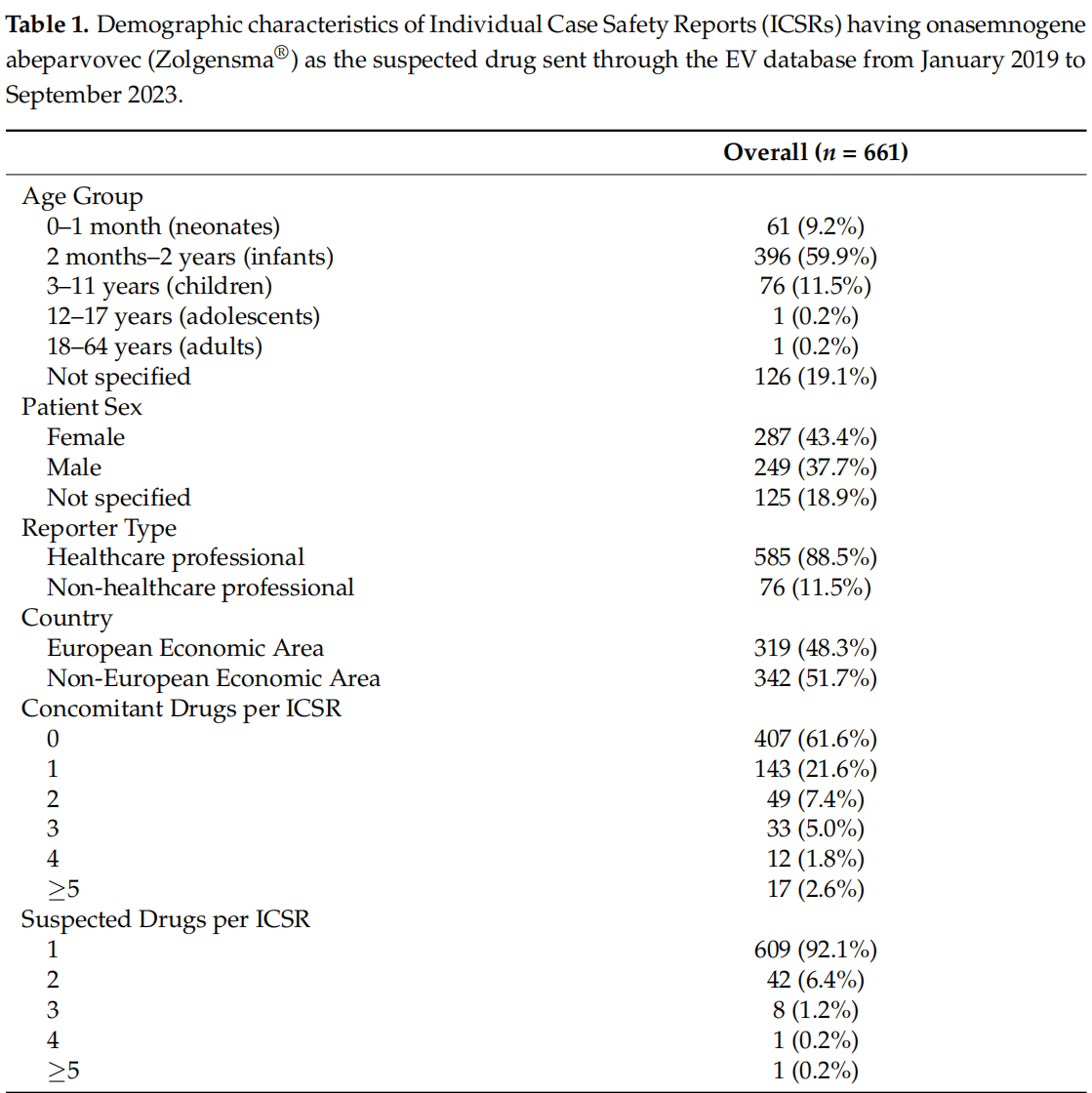
表 1 介绍了患者的人口统计学特征。从各年龄组的 ICSR 分布情况来看,婴儿组(2 个月至 2 岁)的比例较高(396 人;59.9%),其次是儿童组(3 至 11 岁),共 76 例 ICSR(11.5%)。新生儿占 ICSR 总数的 9.2%(n = 61)。在所有病例中,女性患者占 287 例(43.4%),男性患者占 249 例(37.7%)。在 125 份综合病例报告中,患者性别不详。医疗保健专业人员是最具代表性的报告人类型,因为他们提交了 EV 中收集到的大多数与甲氧苄啶相关的 ICSR(88.5%)。大多数 ICSR 仅将 onasemnogene 报告为可疑药物(92.1%),61.6% 的病例未报告伴随药物。泼尼松龙(Prednisolone)和奴西那生(Nusinersen)是其他较多的可疑药物,分别在 26 份(35.1%)和 23 份(31.1%)ICSR 中有所描述。只有一个病例将利地普仑列为疑似药物。所有其他可疑药物及其治疗适应症见补充表 S1。
关于不良反应的严重程度分布,43%的不良反应并不严重(n = 1185),超过 50%的报告不良反应被归类为严重不良反应。其中,严重不良反应主要归类为其他重要医学症状(n = 721;26.3%)。此外,导致/延长患者住院时间或危及生命的严重不良反应分别占 21%(588 例)和 4.3%(118 例)。虽然有 54.7% 的 ADR 结果不明(n = 1502),但大多数报告的结果是好的,结果为康复/解决(n = 676;24.6%)或康复/解决(n = 238;8.7%)。另一方面,有 6.9% 的 ADR 没有解决(n = 188),在所有报告的 ADR 中,有 130 例(4.7%)出现了致命结果(表 2)。这 130 例出现致命结果的 ADR 在 39 份 ICSR 中均有描述,主要涉及 2 个月至 2 岁的患者(n = 33)。只有 1 例致命病例与 0-1 个月大的患者有关,儿童组(3-11 岁)中没有致命病例。有 3 例出现死亡病例的 ICSR 将 Nusinersen 作为另一种可疑药物。我们在补充表 S2 中报告了所有导致死亡的不良事件。致死原因主要是心脏骤停(8 例;6.2%)、呼吸骤停或呼吸衰竭(均为 5 例;3.8%)或急性肝功能衰竭(4 例;3.1%)。
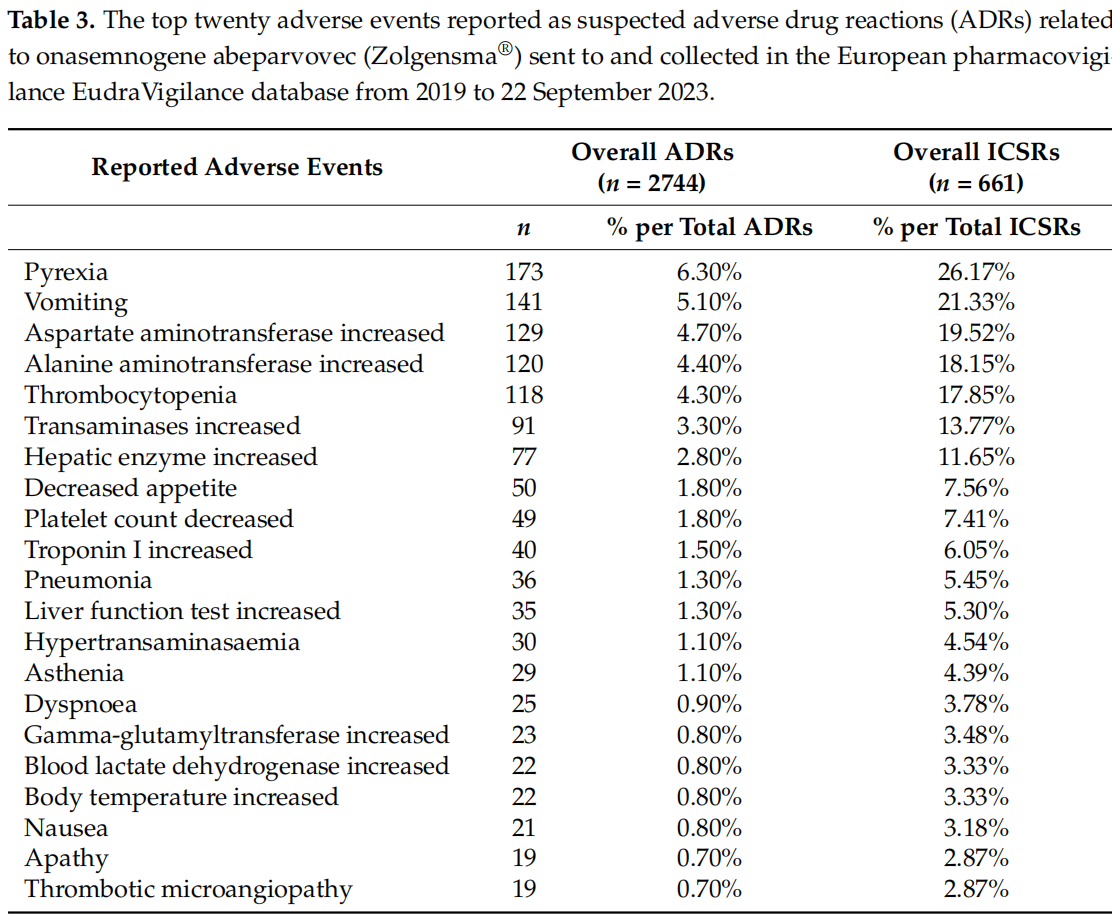
表 3 介绍了最常报告的不良反应,主要包括热病(173 例;6.3%)、呕吐(141 例;5.10%)、天冬氨酸氨基转移酶和丙氨酸氨基转移酶升高(129 例;4.70% 和 120 例;4.40%)以及血小板减少(118 例;4.30%)。在表 3 中,我们还将单个报告的 ADR 与 ICSR 总数进行了比较。然而,如果将那些表示相同临床不良事件但报告者用不同术语报告的 ADR 相加,我们发现有 505 例 ADR 表示肝酶升高,195 例 ADR 表示体温升高,167 例描述血小板计数减少,分别占 ICSR 的 76.40%、29.50% 和 25.26%。
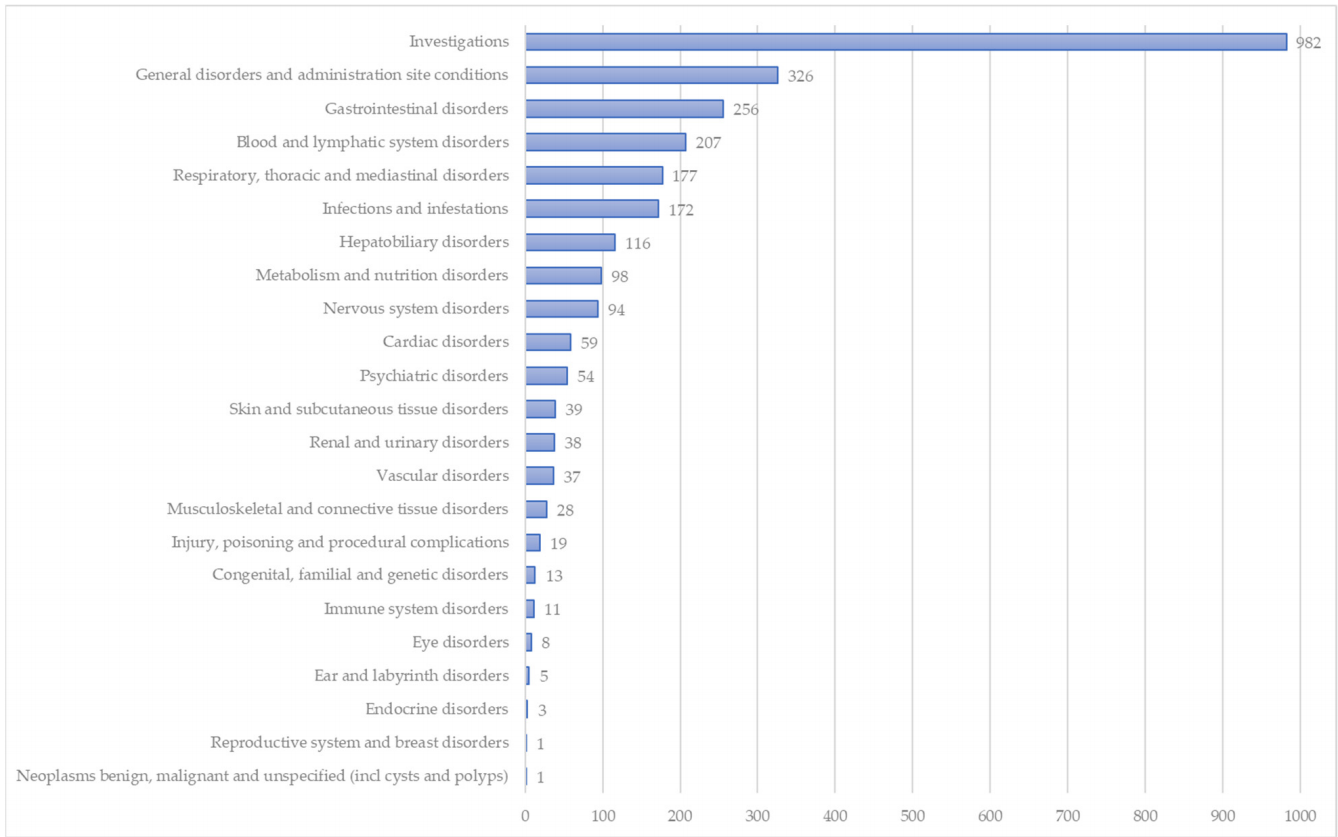
在图 2 中,报告的不良事件按系统器官分类(SOC)。在这些 SOC 中,"检查"(35.8%)、"一般疾病和给药部位状况"(11.9%)、"胃肠道疾病"(9.3%)、"血液和淋巴系统疾病"(7.5%)以及 "呼吸系统、胸部和纵隔疾病"(6.5%)的报告频率较高。
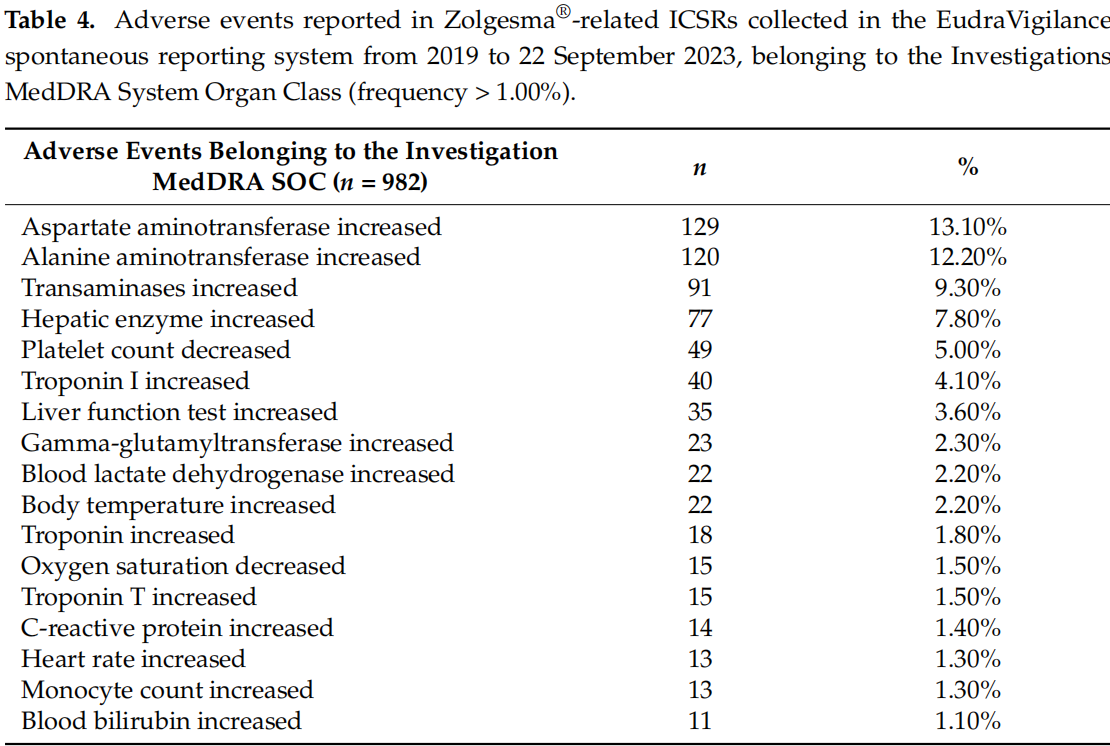
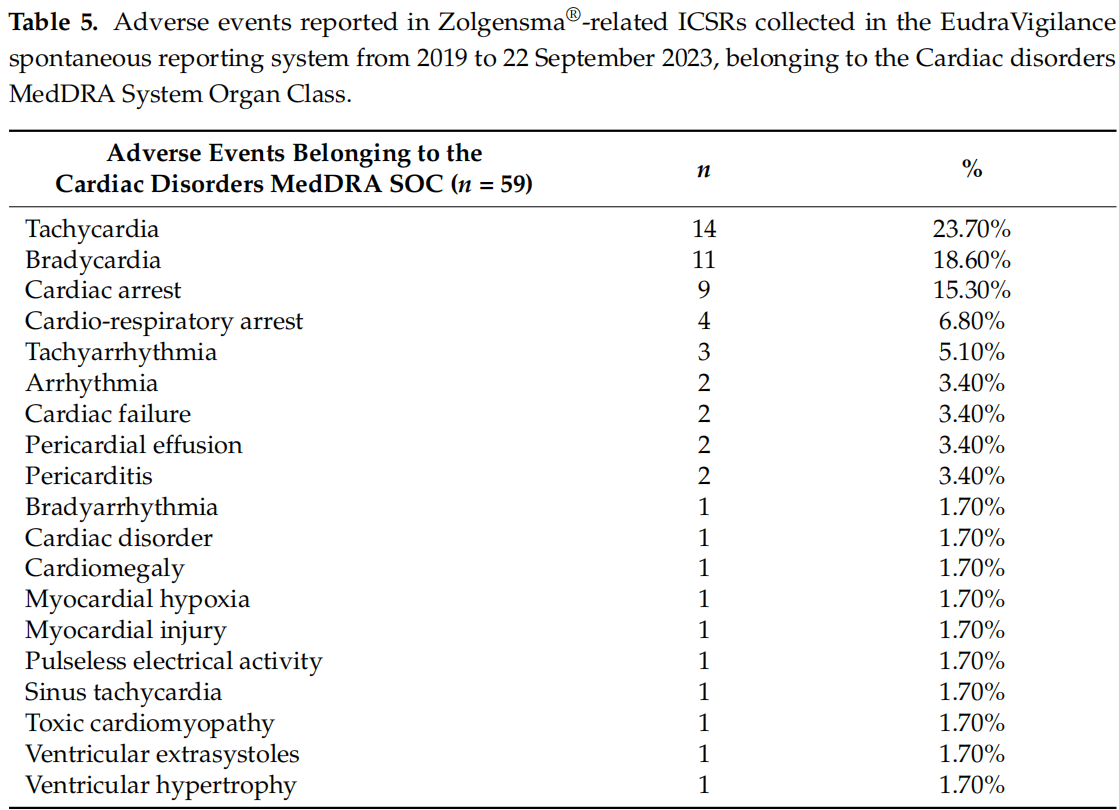
在属于调查 SOC 的事件中(表 4),最常见的是肝脏、造血和心脏临床实验室检查的定性结果。特别是肝功能值升高,如天门冬氨酸和丙氨酸氨基转移酶(129 人和 120 人)、γ-谷氨酰转移酶(23 人)、血胆红素(11 人)或一般肝功能检测值升高(35 人),占调查人数的 40% 以上。血小板计数减少(49 例)和单核细胞计数增加(13 例)是造血功能紊乱的表现。其他变化,如血乳酸脱氢酶(22 例)、肌钙蛋白 I(40 例)和 T(15 例)值升高,则是组织损伤的迹象。最后,心律改变、急性肝功能衰竭和肝细胞溶解分别出现在心脏和肝脏疾病中,如表 5 和表 6 所述。关于肿瘤(良性、恶性或不明原因(包括囊肿和息肉))SOC,只有一份 ICSR 报告了属于此类的不良事件。这是 2 个月至 2 年组中一名男性患者发生的星形细胞瘤恶性肿瘤,导致或延长了他的住院时间,但没有结果。
3. Discussion 3.讨论
Our study aimed to describe the Zolgensma® safety profile emerging from a real-world context by analyzing data collected in the European pharmacovigilance database. Our choice was based on the consideration that, even if pre-marketing clinical trials allow the acquisition of the majority of important drug-safety data, only use in a real-world context can better define the safety aspects, allowing for the identification of rarer ADRs [15,16,17,18]. For these reasons, continuous post-marketing monitoring of drug safety is essential. Long-term safety evaluation is always considered necessary, especially for drugs that have been authorized with conditional and/or accelerated approvals, as often happens for innovative drugs [19,20,21,22]. This necessity is amplified for some particular drug classes, like the orphan ones used for rare diseases [23]. Zolgensma® meets all these mentioned characteristics, as an innovative drug, supported through EMA’s PRIority MEdicines (PRIME) scheme [24], which received a conditional marketing authorization for the rare disease, SMA [24]. The efficacy and safety data obtained in post-marketing can be particularly important for possible confirmation or re-evaluation of a drug’s safety and efficacy profiles and innovativeness, as well as its price [25,26]. Also, this aspect is particularly relevant for Zolgensma®, considering its high cost (approximately $2 million per course of treatment) [27]. However, some pharmacoeconomic studies in the literature support the cost-effectiveness of this gene therapy compared with the other therapeutic possibilities, when used in pre-symptomatic patients [28,29,30,31,32].
我们的研究旨在通过分析欧洲药物警戒数据库中收集的数据,描述佐尔根斯马 ® 在实际应用中的安全性。我们的选择是基于以下考虑:即使上市前临床试验可以获得大部分重要的药物安全性数据,但只有在真实世界中使用才能更好地确定安全性方面的问题,从而识别罕见的不良反应[15, 16, 17, 18]。因此,上市后持续监测药物安全性至关重要。长期的安全性评价总是被认为是必要的,尤其是对于有条件批准和/或加速批准的药物,创新药物也常常如此[19, 20, 21, 22]。对于某些特殊类别的药物,如治疗罕见病的孤儿药,这种必要性就更大了[23]。Zolgensma ® 符合上述所有特征,作为一种创新药物,它在 EMA 的 PRIority MEdicines(PRIME)计划的支持下[24],获得了罕见病 SMA 的有条件上市许可[24]。上市后获得的疗效和安全性数据对于确认或重新评估药物的安全性、疗效、创新性及其价格尤为重要[25, 26]。此外,考虑到 Zolgensma ® 的高昂成本(每个疗程约 200 万美元),这方面的研究也尤为重要 [ 27]。不过,一些文献中的药物经济学研究表明,与其他治疗方法相比,这种基因疗法用于症状出现前的患者时具有成本效益[28, 29, 30, 31, 32]。
From our analysis, 661 safety reports related to Zolgensma® and collected in the European pharmacovigilance database emerged. Excluding the partial data referred to 2023, the annual reporting trend was growing up to 2022. Our reporting trend differed compared with the trend that emerged from a recent study conducted on the US pharmacovigilance database [33]. Following the surge in the Zolgensma®-related ADR reporting in 2020 compared with 2019, the authors found a decreasing trend in the number of reports collected until 2022 in the US database, the Food and Drug Administration Adverse Event Reporting System (FAERS) [33]. Regarding the sex distribution, although some evidence suggests that males may be more vulnerable to SMA than females [34,35], our analysis revealed a greater reporting of ADRs in female patients. This result, as well as the major distribution in terms of the reporter type in favor of HPs, is in line with the analysis conducted by Zhuang et al. on the US database [33]. As described in other studies, HPs represent the major reporting source, even if, to date, citizens can also send safety reports to regulatory authorities [36,37]. The distribution of reports by age group of patients is also comparable, although not completely coincident. Our analysis revealed that the majority of reports referred to patients aged between 2 months and 2 years, while the analysis of FAERS data revealed that the majority of adverse events reported for onasemnogene abeparvovec referred to patients less than 1 year of age. However, this slight discrepancy between the two results could be traced back to the different methods of data extraction and categorization related to the age of the patients. The data extraction method used for the present pharmacovigilance study did not allow us to trace the precise age of the patient, but only the age group to which it referred.
根据我们的分析,欧洲药物警戒数据库共收集了 661 份与佐根斯玛 ® 相关的安全报告。剔除 2023 年的部分数据,直至 2022 年,每年的报告趋势都在增长。我们的报告趋势与最近在美国药物警戒数据库中进行的一项研究[33]得出的趋势有所不同。与 2019 年相比,2020 年与佐尔根斯玛 ® 相关的 ADR 报告数量激增,但作者发现,直到 2022 年,美国数据库--食品药品管理局不良事件报告系统(FAERS)--收集到的报告数量呈下降趋势[ 33]。在性别分布方面,虽然有证据表明男性可能比女性更容易感染 SMA[ 34, 35],但我们的分析表明女性患者的 ADR 报告更多。这一结果以及报告类型的主要分布倾向于 HPs,与 Zhuang 等人对美国数据库的分析结果一致[ 33]。正如其他研究中所描述的,尽管迄今为止公民也可以向监管机构发送安全报告,但高危人群是主要的报告来源[36, 37]。按患者年龄组划分的报告分布情况也具有可比性,尽管并非完全一致。我们的分析显示,大多数报告涉及年龄在 2 个月至 2 岁之间的患者,而 FAERS 数据分析显示,onasemnogene abeparvovec 的大多数不良事件报告涉及年龄小于 1 岁的患者。不过,这两个结果之间的细微差别可能是由于数据提取和与患者年龄相关的分类方法不同造成的。本药物警戒研究采用的数据提取方法无法准确追踪患者的年龄,只能追踪其所属的年龄组。
As regards the types of adverse events, our results were in line with the recently published Zhuang et al. study [33]. Both pharmacovigilance studies highlighted a higher reporting of pyrexia, vomiting, increased aspartate aminotransferase, increased alanine aminotransferase, thrombocytopenia, increased transaminases, and increased liver enzymes, as ADRs related to the SMA gene therapy. Hepatotoxicity, transient thrombocytopenia, and thrombotic microangiopathy have been identified as possible Zolgensma® toxicities [13]. These safety aspects emerged among the top twenty ADRs reported in our dataset. In addition to possible liver damage, signs of cardiac damage also emerged among the most frequently adverse events reported, such as the increase in troponin I. The heart and the liver had also been found to be the main target organs of Zolgensma® toxicity in pre-clinical studies [38]. According to the main safety results derived from non-clinical studies, inflammation, edema, fibrosis, and characteristics of widespread myocardial degeneration/regeneration in the ventricles emerged at the cardiac level in mice. These findings were present at all studied doses and were dose-related in terms of seriousness [38].
关于不良事件的类型,我们的研究结果与最近发表的 Zhuang 等人的研究结果一致[ 33]。这两项药物警戒研究都强调,与 SMA 基因疗法有关的 ADRs 包括热病、呕吐、天门冬氨酸氨基转移酶升高、丙氨酸氨基转移酶升高、血小板减少、转氨酶升高和肝酶升高的报告较多。肝脏毒性、一过性血小板减少和血栓性微血管病已被确定为佐根斯玛 ® 可能出现的毒性反应[13]。在我们的数据集中,这些安全性问题出现在报告的前二十种不良反应中。在临床前研究中,心脏和肝脏也被发现是 Zolgensma ® 毒性的主要靶器官[38]。根据非临床研究得出的主要安全性结果,小鼠心脏出现炎症、水肿、纤维化以及心室广泛的心肌变性/再生特征。在所有研究剂量下都会出现这些结果,而且严重程度与剂量有关[38]。
As regards a possible hepatotoxicity risk, our results confirmed the possible hepatic damage evidenced by increased hepatic enzymes or tests (ALT and AST). This safety aspect, already found in pre-clinical studies [38], emerged from the first patients enrolled in pre-marketing clinical trials [39]. In post-mortem tissue samples from two patients treated with onasemnogene abeparvovec, the highest concentrations of vector DNA were found in the liver [39]. Safety signals have also emerged in the post-marketing context about the liver and heart organs [38]. Similarly, our analysis revealed reports of possible liver damage (hypertransaminasemia, liver disorder, acute liver failure, and liver cytolysis) and cardiac rhythm alterations. The increase in hepatic enzymes can be caused by the immune response induced the gene therapy [40]. Both hepatobiliary and hematologic abnormalities can be considered the immune response to the viral capsid. Moreover, hepatoxicity risk is complicated by the major predisposition of patients with SMA to acute liver injury [39]. Abnormal fatty acid metabolism, as the reported cause of liver failure, was reported in children with SMA [40]. Their increased risk of dyslipidemia and fatty liver could predispose them to hepatotoxicity [41]. Zolgensma®-related hepatoxicity can generally be mitigated with prophylactic prednisolone. This latter emerged among the most frequently reported other concomitant drug in our study. These hepatic and heart rhythm disorders also emerged from the analysis of the US FAERS pharmacovigilance database. Furthermore, it is important to note that, in both studies, a risk of damage to the heart was highlighted, evidenced by an increase in troponin blood concentrations. According to Zhuang et al., such increased levels of troponin I and T have been identified as idiosyncratic adverse reactions to onasemnogene abeparvovec [33]. However, the possible causal relationship and the biological plausibility between onasemnogene abeparvovec treatment and cardiotoxicity is still unclear. An increased risk of cardiac events may be related to SMA itself. Out of all the suspected ADRs reported, some may be symptoms of progression of SMA, as a disease with a very broad and subjective spectrum of symptoms, which also change based on the type of SMA. Heart and liver function should be monitored before, during, and after use of the drug to prevent more serious manifestations. In addition to hepatic and cardiac adverse events, serious respiratory adverse events, such as bronchiolitis, pneumonia, respiratory distress, and respiratory syncytial virus bronchiolitis, were also observed in the STR1VE trial. However, they were considered unrelated to onasemnogene abeparvovec [41]. Pneumonia and dyspnea emerged among the top twenty ADRs in our analysis. Regarding the possible tumorgenicity due to chromosomal integration as a potential Zolgensma® adverse event, only one case describing a tumoral adverse event emerged in our analysis. This potential risk certainly requires more long-term monitoring and careful analysis with more appropriate methodologies. The same applies to the hypothetical risk of dorsal root ganglion toxicity, which is more difficult to identify through pharmacovigilance database analysis. However, none of the retrieved ICSRs involved either areflexia or hyporeflexia, which have emerged in other studies as sensory abnormalities suggestive of gangliopathy [42].
至于可能存在的肝毒性风险,我们的研究结果证实,肝酶或检测指标(谷丙转氨酶和谷草转氨酶)的升高证明可能存在肝损伤。这一安全性在临床前研究[38]中就已发现,上市前临床试验[39]的首批患者也发现了这一点。在接受onasemnogene abeparvovec治疗的两名患者的尸检组织样本中,肝脏中的载体DNA浓度最高[39]。在上市后,肝脏和心脏器官也出现了安全信号[38]。同样,我们的分析显示,有报告称可能存在肝损伤(高转氨酶血症、肝功能紊乱、急性肝衰竭和肝细胞溶解)和心律改变。肝酶的增加可能是由于基因疗法诱导的免疫反应引起的[40]。肝胆和血液学异常都可视为对病毒外壳的免疫反应。此外,由于 SMA 患者极易发生急性肝损伤,肝毒性风险变得更加复杂[39]。据报道,脂肪酸代谢异常是导致 SMA 儿童肝功能衰竭的原因[40]。他们患血脂异常和脂肪肝的风险增加,这可能使他们容易发生肝毒性[41]。Zolgensma ® 与此相关的肝毒性一般可通过预防性泼尼松龙得到缓解。在我们的研究中,后者是最常报告的其他伴随药物之一。对美国 FAERS 药物警戒数据库的分析也发现了这些肝病和心律紊乱。此外,值得注意的是,在这两项研究中,都强调了对心脏造成损害的风险,肌钙蛋白血药浓度的升高就是证明。根据 Zhuang 等人的研究,肌钙蛋白 I 和 T 水平的升高已被确定为 onasemnogene abeparvovec 的特异性不良反应[ 33]。然而,onasemnogene abeparvovec 治疗与心脏毒性之间可能存在的因果关系和生物学合理性仍不清楚。心脏事件风险的增加可能与 SMA 本身有关。在报告的所有疑似不良反应中,有些可能是 SMA 病程进展的症状,因为这种疾病的症状非常广泛且主观,还会根据 SMA 的类型发生变化。应在用药前、用药期间和用药后监测心脏和肝功能,以防止出现更严重的表现。除了肝脏和心脏不良事件外,STR1VE 试验中还观察到严重的呼吸道不良事件,如支气管炎、肺炎、呼吸窘迫和呼吸道合胞病毒支气管炎。不过,这些事件被认为与onasemnogene abeparvovec无关[ 41]。 在我们的分析中,肺炎和呼吸困难出现在前二十种不良反应中。关于染色体整合可能导致的肿瘤致病性这一潜在的佐根玛 ® 不良反应,我们的分析中仅出现了一例描述肿瘤不良反应的病例。这种潜在风险当然需要更多的长期监测,并采用更合适的方法进行仔细分析。背根神经节毒性的假设风险也是如此,这种风险更难通过药物警戒数据库分析来识别。然而,在检索到的 ICSR 中,没有一个涉及反射消失或反射减退,而在其他研究中,反射消失或反射减退是提示神经节病变的感觉异常[ 42]。
Our study showed some strengths as well as some limitations. The use of a low-cost, broad database, coming from the real world setting, overcame several limitations of data collection during the clinical and pre-approval trials, and helped in characterizing drug safety profiles. However, this study also had several limitations, particularly the underreporting phenomenon, which characterizes all the spontaneous reporting systems [43,44,45,46]. This phenomenon can have repercussions for public health, interfering with the ADRs’ incidence quantification and risk estimates, as well as delaying the identification of safety signals. Only 6–10% of all adverse events are reported to regulatory authorities [43,47]. We cannot exclude the fact that some safety cases may not have been reported to the drug authorities and thus not collected in the EV. In addition to the underreporting, possible missing information can also be a difficulty in analysis based on spontaneous reporting systems. The quality of information reported may be incomplete and lack useful clinical information. This can delay a complete evaluation of confounding factors such as clinical history and concomitant comorbidities and medications. From our data source, we also could not retrieve information on the exact dates of administration and event onset—useful for a long-term safety evaluation. Moreover, our data source did not report the exact number of patients exposed to the treatment as real users of Zolgensma®; this would be necessary for reporting-rate evaluation. Considering these limitations, our study only aimed to analyze ICSRs related to Zolgensma® and to show its adverse event characteristics; it refrained from asserting any direct causal association between the SMA gene therapy and the adverse events reported as suspected ADRs. Considering the peculiarities of the rare disease, SMA, further investigations with appropriate methodologies are needed. However, analysis of the post-marketing database often represents the first step or the primum movens in identifying new safety aspects needing deeper examination.
我们的研究显示了一些优势和局限性。使用来自真实世界的低成本、广泛的数据库,克服了临床试验和批准前试验中数据收集的一些局限性,有助于描述药物安全性特征。不过,这项研究也存在一些局限性,特别是所有自发报告系统都存在的漏报现象[43, 44, 45, 46]。这种现象会对公共卫生产生影响,干扰不良反应发生率的量化和风险估计,并延迟安全信号的识别。在所有不良事件中,只有 6-10%向监管机构报告[ 43, 47]。我们不能排除有些安全案例可能没有上报给药品管理部门,因此没有被收集到评价工具中。除报告不足外,可能存在的信息缺失也是基于自发报告系统进行分析的一个难题。报告的信息质量可能不完整,缺乏有用的临床信息。这可能会延误对临床病史、并发症和药物等混杂因素的全面评估。从我们的数据源中,我们也无法检索到用药和事件发生的确切日期--这对长期安全性评估非常有用。此外,我们的数据源没有报告作为佐尔根斯玛实际使用者接受治疗的患者的确切人数 ® ;这对于报告率评估非常必要。考虑到这些局限性,我们的研究仅旨在分析与佐尔金斯玛 ® 相关的 ICSR,并显示其不良事件特征;我们并不断言 SMA 基因疗法与作为疑似 ADR 上报的不良事件之间存在任何直接因果关系。考虑到 SMA 这种罕见疾病的特殊性,需要采用适当的方法进行进一步调查。然而,对上市后数据库的分析往往是发现需要深入研究的新的安全性问题的第一步或首要步骤。
4. Materials and Methods 4.材料与方法
On 22 September 2023, we retrieved data on Individual Case Safety Reports (ICSRs) reporting Zolgensma® as a suspected drug from the EV, the EMA pharmacovigilance database (www.adrreports.eu, accessed on 22 September 2023). This is a publicly available database, that contains the spontaneous safety reports submitted to the EMA [15]. Analysis of pharmacovigilance databases allows for early detection of safety signals and quantification of the association between drugs and reported adverse events (AEs) [16,17]. A wide variety of sources can send safety reports, both healthcare professionals (HPs) (e.g., physicians, pharmacists, and nurses) and non-healthcare professionals (patients, citizens, lawyers, and consumers) [18,19,20,21,22,23]. ICSRs reporting onasemnogene as a suspected drug were searched and a list of cases was exported. Our study period was 1 January 2019–22 September 2023. We checked for duplicates highlighted by the same ICSR code. We conducted an observational retrospective study, verifying the reporting annual trend, the distribution of the reports by sex and age group, the source country, and the reporter type, as well as the number of concomitant or suspected drugs. We analyzed the downloaded data. In the EV, the age groups are categorized as neonates, including preterm and term newborns (0–1 month), infants (2 months–2 years), and children (3–11 years). The reporter types are classified as healthcare professional and non-healthcare professional. The source country is not specified, but it is distinguished as belonging to the European Economic Area or the Non-European Economic Area. The suspected adverse drug reactions (ADRs) were analyzed in terms of seriousness, outcome, and type of event. According to current pharmacovigilance regulations, an ADR is categorized as serious if it induces death, hospitalization or prolongation of hospitalization, severe or permanent disability, threat to life, congenital abnormalities/birth defects, or is considered clinically relevant.
2023 年 9 月 22 日,我们从 EMA 药物警戒数据库 EV( www.adrreports.eu,访问日期:2023 年 9 月 22 日)中检索到了将佐根斯玛 ® 报告为可疑药物的个例安全报告 (ICSR) 数据。这是一个可公开访问的数据库,其中包含自发提交给 EMA 的安全性报告[ 15]。通过分析药物警戒数据库,可以及早发现安全信号,并量化药物与所报告不良事件(AEs)之间的关联[16, 17]。安全报告的来源多种多样,既有医疗保健专业人员(HP)(如医生、药剂师和护士),也有非医疗保健专业人员(患者、公民、律师和消费者)[18, 19, 20, 21, 22, 23]。我们搜索了将安赛蜜作为可疑药物进行报告的 ICSR,并导出了病例列表。我们的研究期限为 2019 年 1 月 1 日至 2023 年 9 月 22 日。我们检查了由相同 ICSR 代码突出显示的重复病例。我们进行了一项观察性回顾研究,核实了报告的年度趋势、按性别和年龄组、来源国和报告人类型分列的报告分布情况,以及伴随药物或可疑药物的数量。我们对下载的数据进行了分析。在 EV 中,年龄组分为新生儿,包括早产儿和足月新生儿(0-1 个月)、婴儿(2 个月-2 岁)和儿童(3-11 岁)。报告人类型分为医护专业人员和非医护专业人员。未说明来源国,但区分为属于欧洲经济区或非欧洲经济区。对疑似药物不良反应(ADR)的严重程度、结果和事件类型进行了分析。根据现行的药物警戒法规,如果药物不良反应导致死亡、住院或住院时间延长、严重或永久性残疾、生命危险、先天性异常/出生缺陷,或被认为与临床相关,则被归类为严重药物不良反应。
In the EV, the reported ADRs are coded according to the Medical Dictionary for Regulatory Activities (MedDRA). We analyzed ADRs based on Preferred Terms (PTs) and corresponding System Organ Class (SOC). We focused on the most representative SOC, and the events belonging to Hepatobiliary disorders and Cardiac disorders SOCs. Since each ICSR can contain more than one ADR, the total number of ADRs can be higher than the overall ICSR number. Moreover, cases with fatal outcomes were investigated as a sub-analysis, describing their distribution in terms of sex and age group, as well as the type of fatal event. All data manipulation and statistical analysis were performed using R Statistical Software (version 4.0.3).
在 EV 中,报告的 ADR 是根据监管活动医学字典 (MedDRA) 进行编码的。我们根据首选术语 (PT) 和相应的系统器官分类 (SOC) 对 ADR 进行了分析。我们重点分析了最具代表性的 SOC,以及属于肝胆疾病和心脏疾病 SOC 的事件。由于每个 ICSR 可能包含一个以上的 ADR,因此 ADR 的总数可能高于 ICSR 的总数。此外,还对出现致命结果的病例进行了子分析,描述了这些病例在性别、年龄组以及致命事件类型方面的分布情况。所有数据处理和统计分析均使用 R 统计软件(4.0.3 版)进行。
5. Conclusions 5.结论
Our study aimed to better define the safety profile of drugs, by using the spontaneous reports of safety data in routine clinical practice. The results of our study confirmed hepatoxicity as the principal issue emerging from Zolgensma® use in clinical practice. Considering that SMA children are predisposed to liver dysfunction, hepatic monitoring is necessary during the treatment. In the same way, cardiac monitoring is also important, considering the possible cardiotoxicity induced by Zolgensma®, even if this latter requires more investigations to better define it and its plausible correlation to the treatment. From our analysis, alterations in the heart rhythm, acute hepatic failure, and hepatic cytolysis emerged among the cardiac and hepatic disorders, respectively.
我们的研究旨在利用日常临床实践中自发报告的安全性数据,更好地界定药物的安全性概况。我们的研究结果证实,肝毒性是在临床实践中使用佐尔根斯玛 ® 时出现的主要问题。考虑到 SMA 儿童容易出现肝功能障碍,因此在治疗期间有必要进行肝功能监测。同样,考虑到佐尔根斯玛 ® 可能诱发心脏毒性,对心脏的监测也很重要,尽管这需要更多的研究来更好地界定心脏毒性及其与治疗的合理相关性。根据我们的分析,心律改变、急性肝功能衰竭和肝细胞溶解分别出现在心脏和肝脏疾病中。
Approval of Zolgensma® for the treatment of SMA has shown evident benefits. Nevertheless, some safety concerns remain unresolved, especially long-term ones. These latter include the potential dorsal root ganglion (DRG) toxicity and late-onset motor dysfunction that emerged as long-term AAV9-mediated SMN overexpression in mouse models [48]. In this context, systematic data collection and long-term follow-up could better define Zolgensma’s long-term safety profile. This is particularly important for the hypothetical tumorgenicity due to chromosomal interaction, which has been identified as an important potential risk. In conclusion, further studies and continuous monitoring are therefore necessary for SMA gene therapy, as an important and expensive therapeutic strategy for a rare disease. The systematic and spontaneous collection of post-marketing data is even more fundamental in the context of such rare diseases and orphan and innovative drugs such as Zolgensma®.
Zolgensma ® 被批准用于治疗 SMA,其疗效显而易见。然而,一些安全性问题仍未得到解决,尤其是长期安全性问题。后者包括潜在的背根神经节(DRG)毒性和晚发性运动功能障碍,这在小鼠模型中长期AAV9介导的SMN过表达时出现[48]。在这种情况下,系统的数据收集和长期随访可以更好地确定 Zolgensma 的长期安全性。这对于染色体相互作用导致的假定肿瘤致病性尤为重要,而染色体相互作用已被确定为一个重要的潜在风险。总之,SMA 基因疗法作为一种治疗罕见病的重要而昂贵的治疗策略,有必要进行进一步研究和持续监测。对于此类罕见病以及孤儿药和创新药(如佐根斯马 ® ),系统、自发地收集上市后数据更为重要。

https://blog.sciencenet.cn/blog-3426442-1434966.html
上一篇:[转载]JEWELFISH 24月结果
下一篇:[转载]Onasemnogene abeparvovec基因疗法治疗症状性婴儿型脊髓性肌萎缩症1型-part1