博文
[转载]Onasemnogene abeparvovec基因疗法治疗症状性婴儿型脊髓性肌萎缩症1型-part2
|||
Onasemnogene abeparvovec基因疗法治疗症状性婴儿型脊髓性肌萎缩症1型
Summary 摘要
Background Spinal muscular atrophy is a rare, autosomal recessive, neuromuscular disease caused by biallelic loss of the survival motor neuron 1 (SMN1) gene, resulting in motor neuron dysfunction. In this STR1VE-EU study, we aimed to evaluate the safety and efficacy of onasemnogene abeparvovec gene replacement therapy in infants with spinal muscular atrophy type 1, using broader eligibility criteria than those used in STR1VE-US. 背景脊髓性肌萎缩症是一种罕见的常染色体隐性神经肌肉疾病,由存活运动神经元1(SMN1)基因的双偶性缺失引起运动神经元功能障碍。在这项 STR1VE-EU 研究中,我们旨在评估 onasemnogene abeparvovec 基因替代疗法对 1 型脊髓性肌萎缩症婴儿的安全性和有效性,采用的资格标准比 STR1VE-US 研究中使用的标准更宽泛。
Methods STR1VE-EU was a multicentre, single-arm, single-dose, open-label phase 3 trial done at nine sites (hospitals and universities) in Italy (n=4), the UK (n=2), Belgium (n=2), and France (n=1). We enrolled patients younger than 6 months (180 days) with spinal muscular atrophy type 1 and the common biallelic pathogenic SMN1 exon 7–8 deletion or point mutations, and one or two copies of SMN2. Patients received a one-time intravenous infusion of onasemnogene abeparvovec (1·1 × 10¹⁴ vector genomes [vg]/kg). The outpatient follow-up consisted of assessments once per week starting at day 7 post-infusion for 4 weeks and then once per month until the end of the study (at age 18 months or early termination). The primary outcome was independent sitting for at least 10 s, as defined by the WHO Multicentre Growth Reference Study, at any visit up to the 18 months of age study visit, measured in the intention-to-treat population. Efficacy was compared with the Pediatric Neuromuscular Clinical Research (PNCR) natural history cohort. This trial is registered with ClinicalTrials.gov, NCT03461289 (completed). 方法 STR1VE-EU是一项多中心、单臂、单剂量、开放标签的3期试验,在意大利(4例)、英国(2例)、比利时(2例)和法国(1例)的9个地点(医院和大学)进行。我们招募了年龄小于6个月(180天)、患有脊髓性肌萎缩症1型、常见双倍致病性SMN1外显子7-8缺失或点突变以及一个或两个SMN2拷贝的患者。患者一次性静脉注射onasemnogene abeparvovec(1-1 × 10¹⁴载体基因组 [vg]/kg)。门诊随访包括从输注后第 7 天起每周评估一次,持续 4 周,然后每月评估一次,直至研究结束(18 个月大或提前终止)。根据世界卫生组织多中心生长参照研究(WHO Multicentre Growth Reference Study)的定义,主要结果是在18个月大之前的任何一次就诊中独立坐立至少10秒钟,并在意向治疗人群中进行测量。疗效与儿科神经肌肉临床研究(PNCR)自然史队列进行了比较。该试验已在 ClinicalTrials.gov 登记,编号为 NCT03461289(已完成)。
Findings From Aug 16, 2018, to Sept 11, 2020, 41 patients with spinal muscular atrophy were assessed for eligibility. The median age at onasemnogene abeparvovec dosing was 4·1 months (IQR 3·0–5·2). 32 (97%) of 33 patients completed the study and were included in the ITT population (one patient was excluded despite completing the study because of dosing at 181 days). 14 (44%, 97·5% CI 26–100) of 32 patients achieved the primary endpoint of functional independent sitting for at least 10 s at any visit up to the 18 months of age study visit (vs 0 of 23 untreated patients in the PNCR cohort; p<0·0001). 31 (97%, 95% CI 91–100) of 32 patients in the ITT population survived free from permanent ventilatory support at 14 months compared with six (26%, 8–44) of 23 patients in the PNCR natural history cohort (p<0·0001). 32 (97%) of 33 patients had at least one adverse event and six (18%) had adverse events that were considered serious and related to onasemnogene abeparvovec. The most common adverse events were pyrexia (22 [67%] of 33), upper respiratory infection (11 [33%]), and increased alanine aminotransferase (nine [27%]). One death, unrelated to the study drug, occurred from hypoxic-ischaemic brain damage because of a respiratory tract infection during the study. 研究结果 2018年8月16日至2020年9月11日,41名脊髓性肌萎缩症患者接受了资格评估。服用onasemnogene abeparvovec时的中位年龄为4-1个月(IQR 3-0-5-2)。33名患者中有32名(97%)完成了研究,并被纳入ITT人群(一名患者尽管完成了研究,但因用药181天而被排除在外)。在 32 名患者中,有 14 名(44%,97-5% CI 26-100)在 18 个月大之前的任何一次就诊中达到了功能性独立坐立至少 10 秒的主要终点(对比 PNCR 队列中 23 名未接受治疗的患者中的 0 人;P<0-0001)。在 ITT 群体中,32 名患者中有 31 名(97%,95% CI 91-100)在 14 个月时无需永久通气支持而存活下来,而在 PNCR 自然史队列中,23 名患者中有 6 名(26%,8-44)在 14 个月时无需永久通气支持而存活下来(P<0-0001)。33例患者中有32例(97%)至少出现过一次不良事件,6例(18%)不良事件被认为是严重的,且与onasemnogene abeparvovec有关。最常见的不良反应是发热(33 例中有 22 例 [67%])、上呼吸道感染(11 例 [33%])和丙氨酸氨基转移酶升高(9 例 [27%])。有一例死亡与研究药物无关,是在研究期间因呼吸道感染导致缺氧缺血性脑损伤。
Interpretation STR1VE-EU showed efficacy of onasemnogene abeparvovec in infants with symptomatic spinal muscular atrophy type 1. No new safety signals were identified, but further studies are needed to show long-term safety. The benefit–risk profile of onasemnogene abeparvovec seems favourable for this patient population, including those with severe disease at baseline. 解读 STR1VE-EU显示,onasemnogene abeparvovec对有症状的1型脊髓性肌萎缩症婴儿有疗效。未发现新的安全性信号,但仍需进一步研究以证明其长期安全性。onasemnogene abeparvovec的获益-风险特征似乎对这一患者群体有利,包括那些基线病情严重的患者。
Participants 与会者
We planned to enrol 30 patients younger than 6 months (180 days) at the time of treatment (day 1) with spinal muscular atrophy type 1 and the common biallelic pathogenic SMN1 exon 7–8 deletion or SMN1 point mutations, and one or two copies of SMN2 (including the known SMN2 gene modifier mutation 859G→ C in exon 7). Patients requiring non-invasive ventilatory support for less than 12 h daily or feeding support (who would have been excluded from STR1VE-US) were eligible. Key exclusion criteria were: previous, planned, or expected scoliosis repair surgery or procedures before age 18 months; requirement of non-invasive ventilatory support for 12 h or more daily in the 2 weeks before dosing; or anti-AAV9 antibody titre of more than 1:50. Full eligibility criteria are listed in the appendix (pp 3–4). 我们计划招募 30 名接受治疗时(第 1 天)年龄小于 6 个月(180 天)的 1 型脊髓性肌萎缩症患者,这些患者患有常见的双倍致病性 SMN1 第 7-8 号外显子缺失或 SMN1 点突变,以及一个或两个 SMN2 拷贝(包括已知的 SMN2 基因修饰突变第 7 号外显子中的 859G→ C)。 每天需要非侵入性通气支持少于 12 小时或喂养支持的患者(这些患者将被排除在 STR1VE-US 之外)均符合条件。主要排除标准包括:曾接受、计划接受或预计接受脊柱侧弯修复手术或在 18 个月前接受手术;用药前 2 周内每天需要 12 小时或更长时间的无创通气支持;或抗 AAV9 抗体滴度超过 1:50。 全部资格标准见附录(第 3-4 页)。
Outcomes 成果
The primary outcome was achievement of the WHO developmental milestone of independent sitting for at least 10 s at any visit up to the 18 months of age study visit, as defined by the WHO Multicentre Growth Reference Study.16 The secondary outcome was ventilation-free survival, defined as the absence of death or permanent ventilation at age 14 months.5,13,14 Permanent ventilation was defined as tracheostomy or the requirement of 16 h or longer daily non-invasive ventilatory support for 14 consecutive days or longer in the absence of acute reversible illness (excluding perioperative ventilation). Assessments of exploratory outcomes, which were WHO and Bayley-III motor milestones,16,18 Bayley-III scales,17 CHOP INTEND scores,7,18 ventilatory support inde- pendence, and ability to thrive (defined by weight greater than the third percentile,19 independence from nutritional support, and normal swallowing function [thin or very thin liquids] at age 18 months), are described in the appendix (p 4). Exploratory motor endpoints were assessed in the efficacy completers population, which included all 33 patients, defined as all treated patients who reached age 14 months for the survival endpoint or age 18 months for achieving the endpoint of sitting without support, or all treated patients who met discontinuation criteria, discontinued the study due to an adverse event, or died. All prespecified exploratory endpoints are reported in the appendix (p 4). Safety was assessed by monitoring adverse events, concomitant medication usage, physical exami- nations, vital signs, cardiac assessments, and laboratory evaluations assessed in the safety population. 5,13,14 长期通气是指气管切开术或在无急性可逆性疾病(不包括围手术期通气)的情况下连续 14 天或更长时间每天需要 16 小时或更长时间的无创通气支持。探索性结果的评估包括 WHO 和 Bayley-III 运动里程碑、16,18 Bayley-III 量表、17 CHOP INTEND 评分、7,18 呼吸支持持续时间和茁壮成长能力(定义为体重大于百分位数第 3 位19 、独立于营养支持、18 个月时吞咽功能正常[稀或极稀液体]),详见附录(第 4 页)。探索性运动终点在疗效完成者人群中进行评估,疗效完成者人群包括所有 33 名患者,即所有治疗后达到 14 个月生存终点或 18 个月达到无需支持坐立终点的患者,或所有治疗后达到中止标准、因不良事件中止研究或死亡的患者。附录(第 4 页)中报告了所有预先指定的探索性终点。安全性通过监测不良事件、伴随药物使用情况、体格检查、生命体征、心脏评估以及安全人群的实验室评估进行评估。
We did a post-hoc analysis of the percentage of patients with similar inclusion criteria to START and STR1VE-US (ie, those who did not require nutritional or ventilatory support, or both at baseline) who achieved independent sitting for at least 10 s and had CHOP INTEND scores of more than 40 or 50 points. 我们对纳入标准与 START 和 STR1VE-US 相似的患者(即基线时不需要营养或呼吸支持或两者都不需要的患者)中实现独立坐立至少 10 秒且 CHOP INTEND 评分超过 40 分或 50 分的患者比例进行了事后分析。
Statistical analysis 统计分析
Primary and secondary efficacy analyses were done in symptomatic patients with biallelic SMN1 deletions and two copies of SMN2 without the genetic modifier, defined as the intention-to-treat population. Primary and secondary outcomes were compared with the PNCR natural history dataset (patients were selected from the PNCR cohort on the basis of STR1VE-EU enrolment criteria), in which none of the patients were able to attain independent sitting and other developmental milestones (rolling over, standing, and walking).2 23 of 337 patients in the PNCR cohort had spinal muscular atrophy onset at age 6 months or younger, biallelic SMN1 deletions, and two copies of SMN2 (appendix p 23). They were not age- matched or sex-matched to the STR1VE-EU cohort at baseline. As a substitute for comparison against a rate of 0 observed in the matched PNCR dataset,2 we assumed that no more than 0·1% of untreated patients with spinal muscular atrophy type 1 achieved independent sitting for at least 10 s at the 18 months of age study visit. The primary outcome was analysed using a one-sample exact binomial test, with a comparison using a fixed threshold of 0·1%. For the secondary analysis of ventilation-free survival at age 14 months, approximately 75% of patients would not survive beyond age 13·6 months (matched PNCR dataset).2 Therefore, a two-sided Fisher’s exact test was used, as prespecified in the statistical analysis plan. The ability to thrive was also analysed using a one-sided exact binomial test with a comparison using a fixed threshold of 0·1%. Other exploratory endpoints are presented only descriptively. For comparison, 95% CIS were estimated using two-sided tests and 97·5% CIs using one-sided tests. Data were analysed using SAS (version 9.4). 主要疗效和次要疗效分析是在有症状的双拷贝SMN1缺失患者和有两个SMN2拷贝但没有基因修饰因子的患者中进行的,这些患者被定义为意向治疗人群。 主要和次要结果与 PNCR 自然病史数据集(根据 STR1VE-EU 入组标准从 PNCR 队列中挑选患者)进行了比较,在 PNCR 队列中,没有一名患者能够达到独立坐立和其他发育里程碑(翻身、站立和行走)2。PNCR 队列中的 337 名患者中,有 23 名脊髓性肌萎缩症患者发病年龄在 6 个月或更小、双拷贝 SMN1 缺失和两个 SMN2 拷贝(附录 P23)。他们与 STR1VE-EU 群体的基线年龄和性别不匹配。作为与匹配的 PNCR 数据集 2 中观察到的 0 率进行比较的替代方法,我们假定在 18 个月大的研究访问中,未接受治疗的 1 型脊髓性肌萎缩症患者中至少有 0-1% 能独立坐立 10 秒。主要结果采用单样本精确二项式检验进行分析,并使用 0-1% 的固定阈值进行比较。对于 14 个月时无通气存活率的次要分析,约 75% 的患者在 13-6 个月后将无法存活(匹配的 PNCR 数据集)。对茁壮成长能力的分析也采用了单侧精确二项检验,并使用 0-1% 的固定阈值进行比较。 其他探索性终点仅以描述性方式呈现。比较时,95% CIS 采用双侧检验,97-5% CI 采用单侧检验。 数据使用 SAS(9.4 版)进行分析。
The study was designed to provide more than 95% power to detect a difference at significance level of α=0·025 using a one-sided exact binomial test for a binomial proportion on the basis of a sample size of at least 25 patients and assumptions from the matched PNCR dataset2 and START study data.5,13 Vital signs, shown as descriptive data, were identified as clinically significant if they met prespecified criteria (appendix p 4). Four categories of adverse events of special interest were predefined: hepatotoxicity, thrombo- cytopenia, cardiac adverse events, and sensory abnormalities suggestive of ganglionopathy. Adverse reports were coded using an industry standardised MedDRA coding dictionary (version 23.0), and adverse events of special interest were classified using specific predefined MedDRA terms. This study is registered with ClinicalTrials.gov, NCT03461289 (completed). 该研究的设计是为了在 α=0-025 的显著性水平上提供超过 95% 的检测差异的能力,采用的是二项比例的单侧精确二项检验,以至少 25 名患者的样本量为基础,并根据匹配的 PNCR 数据集2 和 START 研究数据进行假设。预设了四类特别关注的不良事件:肝毒性、血栓性细胞减少症、心脏不良事件和提示神经节病变的感觉异常。 不良反应报告使用行业标准化的 MedDRA 编码字典(23.0 版)进行编码,特别关注的不良反应事件使用预先定义的特定 MedDRA 术语进行分类。本研究已在 ClinicalTrials.gov 注册,编号为 NCT03461289(已完成)。
Results 成果
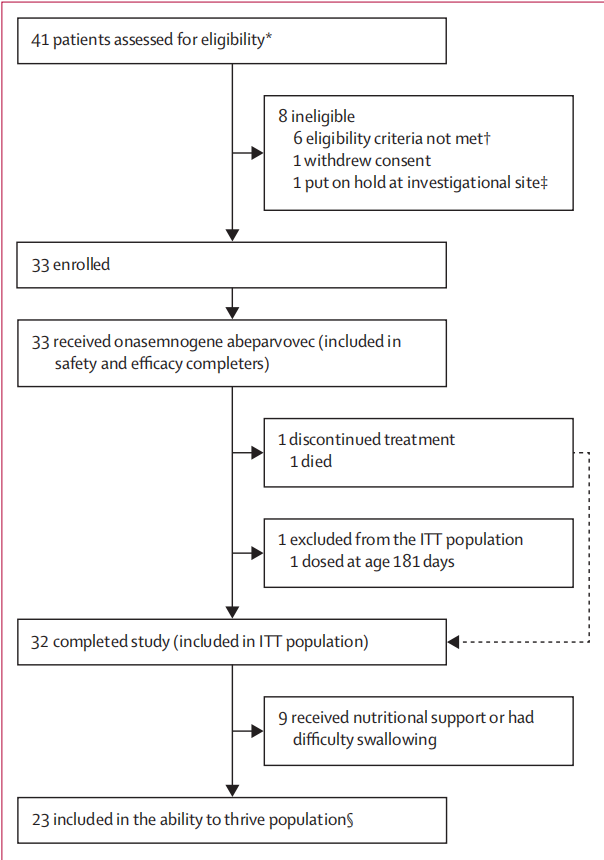
From Aug 16, 2018, to Sept 11, 2020, 41 patients with spinal muscular atrophy type 1 were assessed for eligibility. 33 patients received one-time onasemnogene abeparvovec and were included in the safety population (figure 1). Eight patients did not meet eligibility criteria (n=6), withdrew consent (n=1), or did not pass screening because enrolment was put on hold at the investigational site and the patient was nearing the upper age limit for enrolment (n=1; re-screened and dosed at a different investigational site). Although we planned to enrol 30 patients, three more patients were already in the enrolment pool when the target recruitment was reached, and they were included in the study for compassionate reasons on the basis of results from START. 32 (97%) of 33 patients completed the study and were included in the ITT population (one patient was excluded despite completing the study because of dosing at 181 days). One patient died at age 6·9 months but was still included in the analysis. 2018年8月16日至2020年9月11日,41名1型脊髓性肌萎缩症患者接受了资格评估。33名患者接受了一次性onasemnogene abeparvovec治疗,并被纳入安全人群(图1)。 8名患者不符合资格标准(n=6)、撤回同意(n=1),或因研究机构暂停入组而未通过筛查,且患者已接近入组年龄上限(n=1;在不同研究机构重新筛查和用药)。虽然我们计划招募 30 名患者,但在达到招募目标时,又有 3 名患者已在招募库中,根据 START 的结果,出于同情原因,他们被纳入了研究。33 名患者中有 32 人(97%)完成了研究,并被纳入 ITT 人群(一名患者尽管完成了研究,但因在 181 天时用药而被排除在外)。一名患者在 6-9 个月大时死亡,但仍被纳入分析。
Because of the impact of the COVID-19 pandemic, any efficacy data collected outside of the statistical analysis plan window (defined as the 18 months of age study visit [>570 days]) were grouped into age 19 months or older. Hypothesis testing was based on data collected up to the 18 months of age study visit. 由于 COVID-19 大流行的影响,在统计分析计划窗口(定义为 18 个月的研究访问[>570 天])之外收集的任何疗效数据都被归入 19 个月或更大的年龄组。假设检验以 18 个月前的研究访问数据为基础。
Baseline characteristics are shown in table 1. The median age at onasemnogene abeparvovec dosing was 4·1 months (IQR 3·0–5·2). All 33 patients had two SMN2 copies and were symptomatic with a variable degree of severity, as shown by baseline CHOP INTEND scores (table 1). None of the patients had the SMN2 modifier mutation. Nine (27%) of 33 received ventilatory support and nine (27%) received feeding support. Of these, five (15%) received both ventilatory and feeding support. 基线特征见表 1。 服用onasemnogene abeparvovec时的中位年龄为4-1个月(IQR为3-0-5-2)。根据基线CHOP INTEND评分(表1),所有33名患者均有两个SMN2拷贝,且症状轻重不一。所有患者均无 SMN2 修饰符突变。33 名患者中有 9 人(27%)接受呼吸支持治疗,9 人(27%)接受喂养支持治疗。其中,5人(15%)同时接受呼吸和喂养支持。
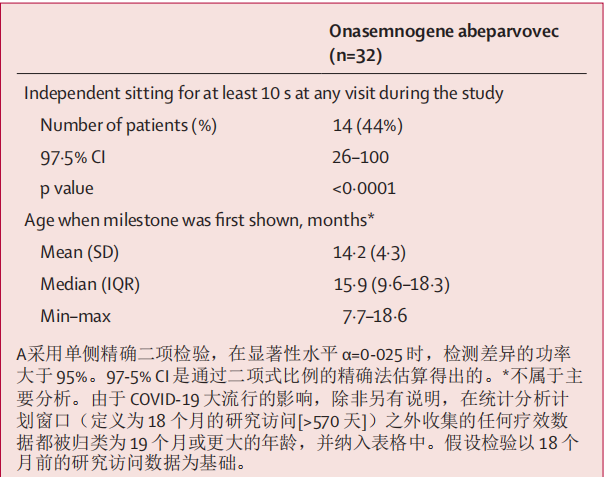
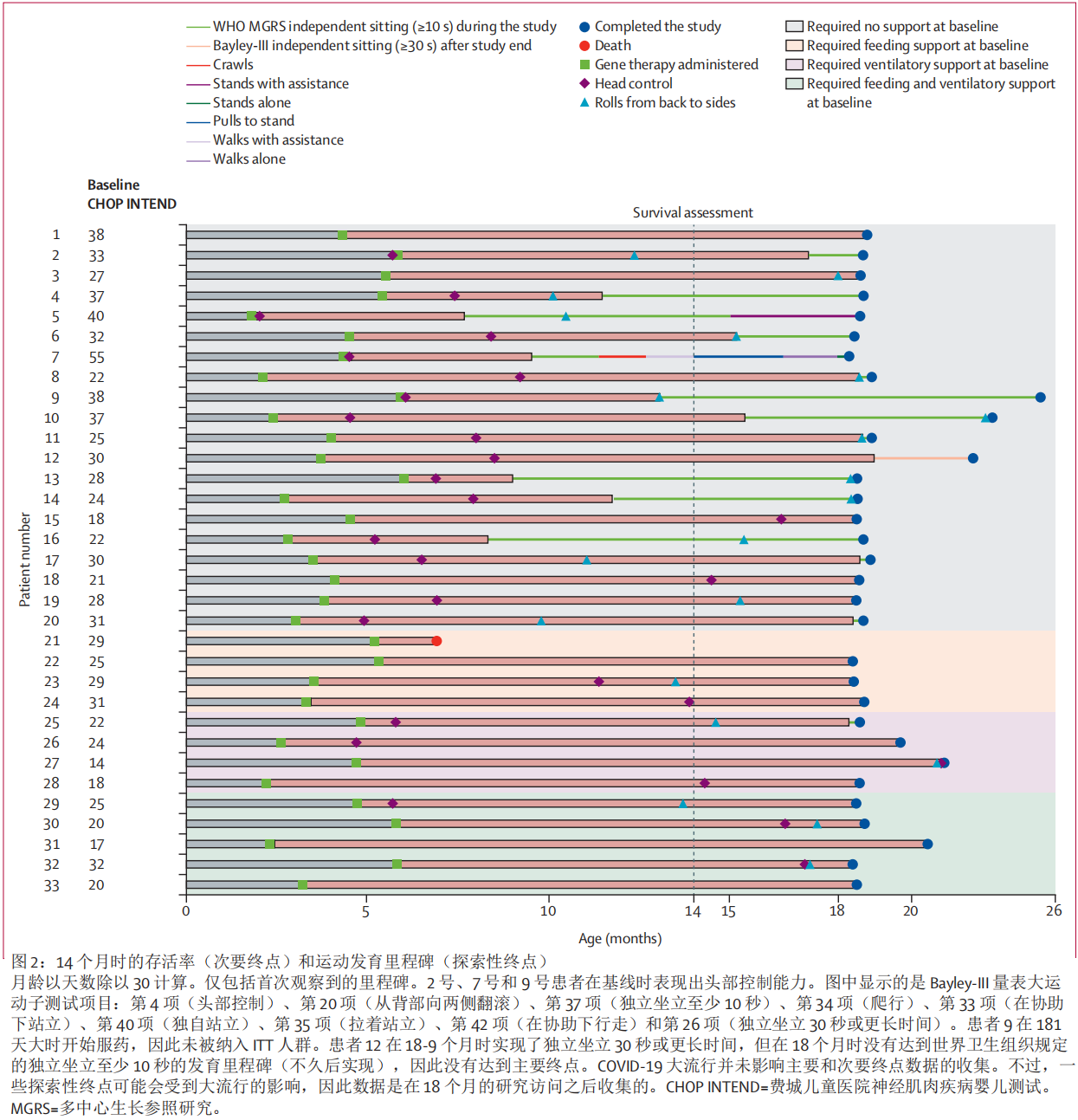
14 (44%, 97·5% CI 26–100) of 32 patients in the ITT population achieved the primary endpoint of functional independent sitting for at least 10 s at any visit up to the 18 months of age study visit (vs 0 of 23 untreated patients in the PNCR cohort; p<0·0001; table 2). Functional independent sitting was observed at a median age of 15·9 months (IQR 9·6–18·3). The patient dosed at day 181 who was excluded from the ITT population also achieved the primary outcome. In a post-hoc analysis of patients with similar inclusion criteria to START and STR1VE-US (ie, those who did not require nutritional or ventilatory support at baseline), 14 (70%) of 20 achieved independent sitting for at least 10 s (figure 2; appendix pp 7–10). Patient 12 achieved independent sitting for 30 s or longer at 18·9 months but did not achieve the WHO developmental milestone of functional independent sitting for at least 10 s at 18 months (achieved shortly afterwards), and thus did not achieve the primary endpoint. 在 ITT 群体的 32 名患者中,有 14 人(44%,97-5% CI 26-100)在 18 个月大之前的任何一次就诊中都达到了功能性独立坐立至少 10 秒的主要终点(PNCR 队列的 23 名未治疗患者中只有 0 人达到这一终点;P<0-0001;表 2)。 中位年龄为 15-9 个月(IQR 9-6-18-3)时,可观察到功能性独立坐姿。 ITT人群中被排除在外的第181天用药患者也达到了主要结果。在对纳入标准与 START 和 STR1VE-US 相似的患者(即基线时不需要营养或通气支持的患者)进行的事后分析中,20 名患者中有 14 名(70%)实现了独立坐立至少 10 秒(图 2;附录第 7-10 页)。患者 12 在 18-9 个月时实现了 30 秒或更长时间的独立坐立,但在 18 个月时没有达到世界卫生组织的发育里程碑,即至少 10 秒的功能性独立坐立(不久后实现),因此没有达到主要终点。
Analysis of the secondary outcome showed that 31 (97%, 95% CI 91–100) of 32 patients in the ITT population survived free from permanent ventilatory support at 14 months compared with six (26%, 8–44) of 23 patients in the PNCR natural history cohort (p<0·0001; appendix p 21).2 The patient who was excluded from the ITT population also survived and was free from ventilatory support at 14 months. 对次要结果的分析表明,在 ITT 群体的 32 名患者中,有 31 人(97%,95% CI 91-100)在 14 个月后存活下来,不再需要永久性通气支持,而在 PNCR 自然病史队列的 23 名患者中,有 6 人(26%,8-44)存活下来(P<0-0001;附录 P 21)2。
Additionally, improvements in motor function were evaluated in the safety and efficacy completers population using prespecified exploratory motor endpoints. 27 (82%) of 33 patients achieved at least one motor milestone during the study (appendix pp 7–10). 23 (77%) of 30 patients achieved head control (three already had head control at baseline), and 19 (58%) of 33 patients rolled from back to sides. 16 (48%) of 33 patients sat without support for 30 s or longer, including 15 (45%) patients (ie, 14 of 32 patients from the ITT population plus one patient dosed at 181 days) who met the primary endpoint of independent sitting for at least 10 s. Patient 5 stood with assistance and patient 7 crawled,walked with assistance, pulled to stand, and walked alone by age 18 months (figure 2; appendix pp 7–10). Two patients achieved milestones such as head control (patient 27) and rolls from back to sides (patients 10 and 27) after age 19 months. 此外,还使用预先指定的探索性运动终点对安全性和疗效完成人群的运动功能改善情况进行了评估。研究期间,33 名患者中有 27 人(82%)达到了至少一个运动里程碑(附录第 7-10 页)。 30名患者中有23名(77%)实现了头部控制(其中3名患者在基线时已经实现了头部控制),33名患者中有19名(58%)实现了从背部向两侧翻滚。 33 名患者中有 16 名(48%)在无支持的情况下坐了 30 秒或更长时间,其中 15 名(45%)患者(即 ITT 组 32 名患者中的 14 名加上一名用药 181 天的患者)达到了独立坐至少 10 秒的主要终点。 两名患儿在 19 个月大后达到了控制头部(患儿 27)和从背部向两侧翻滚(患儿 10 和 27)等里程碑。
Rapid and sustained mean increases in total CHOP INTEND score from baseline of 6·0 points (SD 5·4) at 1 month, 10·3 points (6·3) at 3 months, and 13·6 points (6·6) at 6 months were reported (appendix p 26). 24 (73%) of 33 patients achieved a CHOPINTEND score of40 points or higher, 14 (42%) achieved a score 50 points or higher, and three (9%) achieved 58 points or higher (appendix p 27). In a post-hoc analysis, the percentage of patients achieving scores higher than 40–50 was greater for patients who were independent from respiratory and feeding support at baseline (18 [90%] of 20) than for those who required support (seven [54%] of 13; appendix p 27). These results differed from those in the PNCR cohort, in which one (4%) of23 patients achieved a CHOPINTEND score of40 points or higher, a score rarely achieved in natural history and almost never maintained.2 By age 18 months, most patients had improvements in raw Bayley-III scale gross motor and fine motor subtests. Mean scale scores of the Bayley-III gross and fine motor subdomains were maintained beyond age 4 months (appendix p 28). 据报告,CHOP INTEND 总分与基线相比出现了快速而持续的平均增长,1 个月时为 6-0 分(SD 5-4),3 个月时为 10-3 分(6-3),6 个月时为 13-6 分(6-6)(附录 p 26)。33 名患者中有 24 人(73%)的 CHOPINTEND 评分达到 40 分或以上,14 人(42%)达到 50 分或以上,3 人(9%)达到 58 分或以上(附录 p 27)。在一项事后分析中,基线时独立于呼吸和喂养支持的患者(20 人中有 18 人 [90%])达到 40-50 分以上的比例高于需要支持的患者(13 人中有 7 人 [54%];附录第 27 页)。这些结果与 PNCR 队列中的结果不同,在 PNCR 队列中,23 名患者中有 1 人(4%)的 CHOPINTEND 得分为 40 分或更高,而这一分数在自然病史中很少达到,而且几乎从未保持过。Bayley-III 评分表粗大运动和精细运动子域的平均分在 4 个月后仍能保持(附录第 28 页)。
Patients had improved respiratory function compared with the natural history cohort; 13 (39%) of 33 patients remained independent of daily ventilatory support (invasive or non-invasive) at age 18 months (vs 0 of 23 patients in the PNCR cohort; p<0·0001). Of nine patients who required non-invasive ventilatory support at baseline, seven still required support at the end of this study, whereas two no longer required ventilatory support (appendix p 21). Of 24 patients who did not require ventilatory support at baseline, 16 patients remained free from ventilatory support at the end of the study. Two patients required transient invasive ventilatory support (endotracheal intubation) for upper respiratory tract illness. 与自然病史队列相比,患者的呼吸功能有所改善;33 名患者中有 13 人(39%)在 18 个月大时仍不需要日常通气支持(有创或无创)(PNCR 队列的 23 名患者中只有 0 人需要;P<0-0001)。在基线时需要无创通气支持的 9 名患者中,有 7 人在研究结束时仍需要支持,而有 2 人不再需要通气支持(附录第 21 页)。 在基线时不需要通气支持的 24 名患者中,有 16 名患者在研究结束时仍然不需要通气支持。两名患者因上呼吸道疾病需要短暂的侵入性通气支持(气管插管)。
Seven (30%, 97∙5% CI 13–100) of 23 patients met the criteria of ability to thrive at age 18 months (vs 0 of 23 patients in the PNCR cohort; p<0·0001; appendix pp 4, 11). Improvements in each component of the ability to thrive composite exploratory endpoint were also observed. 15 (65%) of 23 patients maintained weight consistent with their age at age 18 months (appendix pp 11, 25). From the nine (27%) of 33 patients who required feeding support at baseline, four were free from feeding support at age 18 months (appendix p 22). 20 (87%) of 23 patients in the ability to thrive population remained free from mechanical feeding support, and nine (39%) could tolerate thin liquids at age 18 months (appendix p 11). 23 名患者中有 7 名(30%,975% CI 13-100)在 18 个月大时达到了茁壮成长能力标准(与 PNCR 队列的 23 名患者中的 0 名相比;P<0-0001;附录 pp 4、11)。此外,还观察到茁壮成长综合探索性终点的各组成部分均有所改善。23 名患者中有 15 名(65%)在 18 个月大时保持了与其年龄相符的体重(附录 pp 11、25)。33 名患者中有 9 人(27%)在基线时需要喂养支持,其中 4 人在 18 个月大时无需喂养支持(附录第 22 页)。在 23 名有茁壮成长能力的患者中,有 20 人(87%)在 18 个月大时仍无需机械喂养支持,有 9 人(39%)在 18 个月大时可以耐受稀薄流质食物(附录第 11 页)。
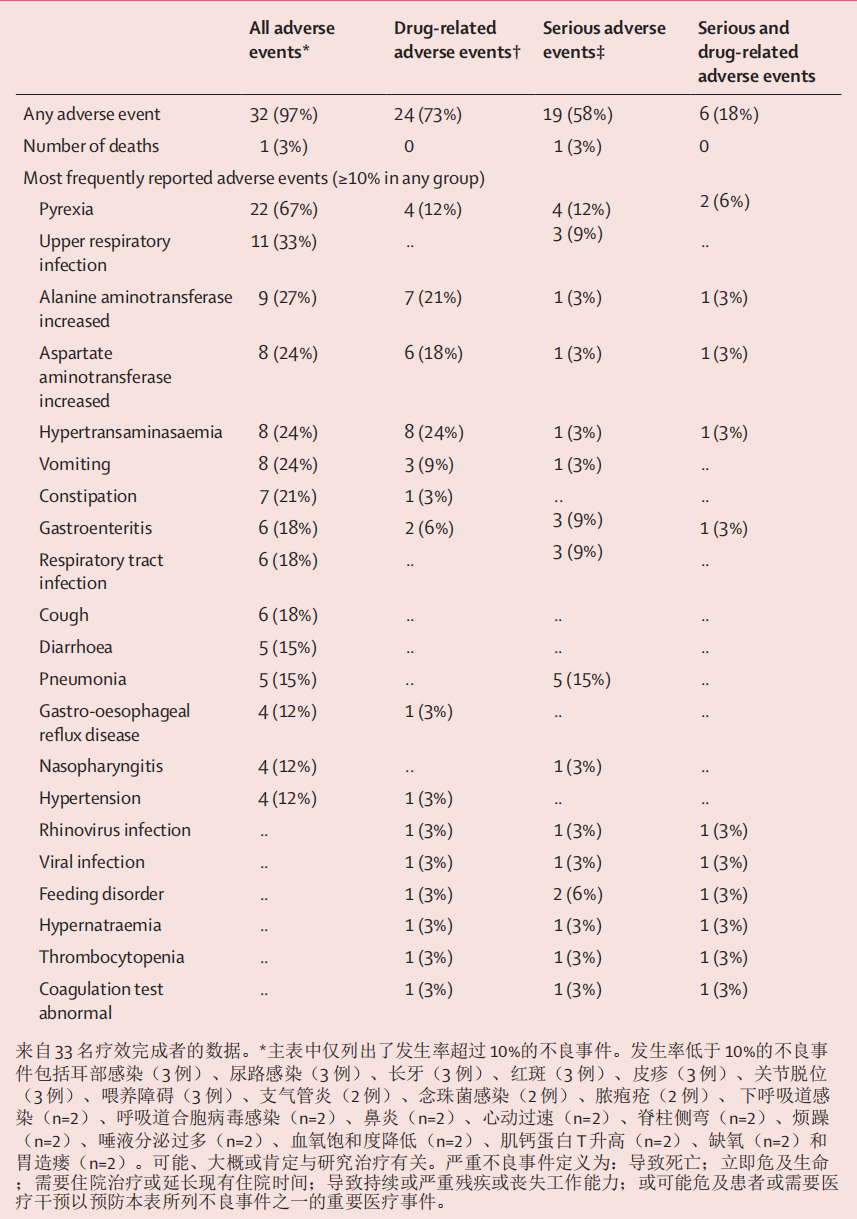
32 (97%) of 33 patients had at least one adverse event and six (18%) had adverse events that were considered serious and related to onasemnogene abeparvovec by the investigator (table 3). The most common adverse events were pyrexia (22 [67%] of 33), upper respiratory infection (11 [33%]), and increased alanine aminotransferase (nine [27%]). One death occurred in the study, with autopsy data confirming that the cause of death was hypoxic- ischaemic brain damage due to a respiratory tract infection resulting from spinal muscular atrophy type 1. The death was considered by the investigator and sponsor to be unrelated to the study drug. 33 名患者中有 32 人(97%)至少出现过一次不良反应,6 人(18%)的不良反应被研究者认为是与 onasemnogene abeparvovec 有关的严重不良反应(表 3)。最常见的不良反应是发热(33 例中有 22 例 [67%])、上呼吸道感染(11 例 [33%])和丙氨酸氨基转移酶升高(9 例 [27%])。研究中出现了一例死亡病例,尸检数据证实死因是 1 型脊髓性肌肉萎缩症导致的呼吸道感染引起的缺氧缺血性脑损伤。研究者和赞助商认为该死亡与研究药物无关。
Of four predefined adverse events (appendix p 12), 28 hepatotoxicity events were reported in 18 (55%) of 33 patients. All adverse events of special interest had asymptomatic laboratory findings (increased alanine and aspartate aminotransferase, and γ glutamyltransferase, or hypertransaminasaemia), except one patient who had elevated alkaline phosphatase and one with hepatic steatosis (and concurrent increased alanine and aspartate aminotransferase; appendix pp 13–18). 12 (36%) of 33 patients had elevations in liver function tests that were not reported as adverse events. 29 (88%) patients had elevated alanine and aspartate aminotransferase, γ glutamyltransferase, or bilirubin at the end of the study, compared with 22 (67%) at baseline. None of the adverse events or laboratory findings were associated with clinical signs or symptoms and most resolved with use or dose modification of prednisolone (appendix pp 14–18). 在四种预定义的不良事件(附录 P12)中,33 例患者中有 18 例(55%)报告了 28 例肝毒性事件。 除了一名碱性磷酸酶升高的患者和一名肝脏脂肪变性的患者(同时丙氨酸和天门冬氨酸氨基转移酶升高;附录 pp 13-18)外,所有特别值得关注的不良事件都有无症状的实验室检查结果(丙氨酸和天门冬氨酸氨基转移酶、γ 谷氨酰基转移酶或高转氨酶血症升高)。 33 例患者中有 12 例(36%)肝功能检测结果升高,但未作为不良事件报告。 29名(88%)患者在研究结束时出现丙氨酸和天门冬氨酸氨基转移酶、γ谷氨酰转移酶或胆红素升高,而基线值为22名(67%)。所有不良事件或实验室检查结果均与临床体征或症状无关,且大多数不良事件或结果在使用或调整泼尼松龙剂量后即可缓解(附录第 14-18 页)。
Five thrombocytopenia-related adverse events were reported (appendix p 19). With one exception, the events (ie, blood urine present, haemoglobin decreased, contusion, or stoma site haemorrhage) were considered unrelated to onasemnogene abeparvovec. The patient who died had thrombocytopenia, which was considered related to treatment and resolved. Three patients had platelet values lower than the prespecified value of 75 × 10⁹ platelets per L. Nadir platelet values were 4–56 × 10⁹ platelets per L (onset on days 1–8 after dosing) and resolved without intervention in all patients (except for the patient who died). 报告了 5 起与血小板减少有关的不良事件(附录第 19 页)。除一例外,其他事件(即出现血尿、血红蛋白下降、挫伤或造口部位出血)均被认为与 onasemnogene abeparvovec 无关。死亡患者的血小板减少被认为与治疗有关,并已缓解。3名患者的血小板值低于每升75×10⁹血小板的预设值。最低血小板值为每升4-56×10⁹血小板(用药后第1-8天出现),所有患者(死亡患者除外)的血小板值均在未干预的情况下得到缓解。
Five patients presented with adverse events that were identified within the cardiac adverse event category. Nine of 13 cardiac adverse events were unrelated to onasemnogene abeparvovec (eg, tachycardia, loss of consciousness, bradycardia, dyspnoea, and increased blood creatine phosphokinase–MB) and eight resolved without intervention (appendix p 20). Events considered possibly related to the study drug included tachycardia (one event in one patient), elevated troponin T (two events in two patients), and increased creatine phosphokinase–MB (one event in one patient). Two patients had laboratory elevations in troponin I with onset at 290 days after dosing; these elevations were not associated with clinical signs or symptoms. 五名患者出现的不良事件属于心脏不良事件类别。13 例心脏不良事件中有 9 例与 onasemnogene abeparvovec 无关(如心动过速、意识丧失、心动过缓、呼吸困难和血肌酸磷酸激酶-MB 增高),8 例在未进行干预的情况下得到缓解(附录第 20 页)。被认为可能与研究药物有关的事件包括心动过速(一名患者发生一次)、肌钙蛋白 T 升高(两名患者发生两次)和肌酸磷酸激酶-MB 增高(一名患者发生一次)。两名患者在用药后 290 天出现肌钙蛋白 I 实验室升高;这些升高与临床体征或症状无关。
Echocardiogram data did not identify intracardiac thrombosis or cardiac dysfunction on the basis of left- ventricular ejection fraction values. Neurological examination at baseline showed clinical signs consistent with spinal muscular atrophy type 1. No additional neurological examination findings sug- gestive of sensory ganglionopathy were identified at follow-up visits. 根据左心室射血分数值,超声心动图数据并未发现心内血栓或心脏功能障碍。 基线神经系统检查显示临床症状与脊髓性肌萎缩症 1 型一致。在随访中,没有发现其他神经系统检查结果提示感觉神经节病变。
Except for low weight, none of the patients had persistently unusual vital signs; those observed were transient and resolved. Despite a high incidence of increased diastolic and systolic blood pressure, four hypertension treatment-emergent adverse events were reported for four patients; one of these events was considered severe but resolved within 2 days. 除体重偏轻外,没有患者出现持续的生命体征异常;观察到的生命体征异常都是一过性的,并已缓解。 尽管舒张压和收缩压升高的发生率很高,但有四名患者报告了四次高血压治疗引发的不良事件;其中一次被认为是严重的,但在两天内就缓解了。
Following the recommendation to increase prophylactic prednisolone dosing for the first 3 days from 1 to 2 mg/kg per day, nine (27%) patients received an initial dose of 2 mg/kg per day. The duration of prednisolone dosing ranged from 54 to 235 days (median 65·0 [IQR 13·0]; mean 80·9 [SD 41·2]) and mean daily dose ranged from 0·5 to 1·6 mg/kg per day. Two patients switched to an equivalent dose of hydrocortisone (using a conversion ratio of 1:4) as an alternative to prednisolone on day 165 and day 132 (extended use after the tapering period was prescribed to treat elevated liver enzymes). 根据将前 3 天的预防性泼尼松龙剂量从每天 1 毫克/千克增加到 2 毫克/千克的建议,9 名患者(27%)的初始剂量为每天 2 毫克/千克。泼尼松龙用药时间从 54 天到 235 天不等(中位数 65-0 [IQR 13-0];平均数 80-9 [SD 41-2]),平均每日剂量从 0-5 到 1-6 毫克/千克不等。两名患者分别在第 165 天和第 132 天改用同等剂量的氢化可的松(转换比为 1:4)替代泼尼松龙(减量期结束后继续使用,以治疗肝酶升高)。
Discussion 讨论
With broader eligibility criteria for nutritional or respiratory function at baseline than STR1VE-US, this STR1VE-EU study was designed to evaluate the safety and efficacy of onasemnogene abeparvovec for a wider range of patients observed in clinical practice. Some patients had more advanced disease at baseline than did those included in STR1VE-US.14 Onasemnogene abeparvovec showed clinically significant efficacy in patients with spinal muscular atrophy type 1, and a safety profile consistent with previously reported results. 与 STR1VE-US 研究相比,STR1VE-EU 研究的基线营养或呼吸功能资格标准更为宽泛,旨在评估 onasemnogene abeparvovec 对临床实践中观察到的更多患者的安全性和有效性。 14 Onasemnogene abeparvovec 对 1 型脊髓性肌萎缩症患者具有显著的临床疗效,其安全性与之前报道的结果一致。
Symptom onset was similar for STR1VE-EU and STR1VE-US,14 and consistent with onset previously reported for spinal muscular atrophy type 1. Compared with STR1VE-US, in which none of the patients required feeding or ventilatory support at baseline,14 some patients in STR1VE-EU required this type of support. Additionally, baseline CHOPINTEND scores were lower in STR1VE-EU (median 28·0 points [IQR 22–32]) than in STR1VE-US (median 33·5 points [24–38]). STR1VE-EU和STR1VE-US的发病症状相似14,与之前报道的1型脊髓性肌萎缩症的发病症状一致。在 STR1VE-US 中,没有患者在基线时需要进食或通气支持,14 而在 STR1VE-EU 中,一些患者需要此类支持。此外,STR1VE-EU 的基线 CHOPINTEND 评分(中位数 28-0 分 [IQR 22-32])低于 STR1VE-US(中位数 33-5 分 [24-38])。
Permanent ventilation-free survival in this STR1VE-EU study was similar to that observed in previous studies.5,13,14 Most patients were alive and free of permanent ventilation at age 14 months, a substantial improvement compared with the natural history cohort. 在这项 STR1VE-EU 研究中,无永久通气存活率与之前研究中观察到的存活率相似。
Although the follow-up was shorter for STR1VE-EU than for START,5,13 most patients in STR1VE-EU achieved developmental motor milestones. Independent sitting for at least 10 s was achieved and maintained by 15 (45%) of 33 patients (ie, 14 of 32 patients from the ITT population plus one patient dosed at 181 days). Sitting was achieved more frequently by patients who did not require ventilatory or feeding support at baseline, which is similar to the STR1VE-US study. Moreover, three patients achieved independent sitting within the WHO normal developmental window (3·8–9·2 months19); four also achieved the Bayley-III independent sitting milestone within the WHO normal developmental window. Our results show that, although motor milestone development in patients with symptomatic spinal muscular atrophy type 1 given onasemnogene abeparvovec might be delayed,5,13,14 sitting independently is achievable. Patients with more severe signs who required nutritional or respiratory support at the time of treatment acquired milestones, such as rolling or head control, at a later age than did those with no requirement for nutritional and respiratory support. A longer follow- up period will help to understand whether further milestones, such as sitting, can be achieved after 18 months. 虽然STR1VE-EU的随访时间比START短5,13,但STR1VE-EU的大多数患者都达到了运动发育的里程碑。 33 名患者中有 15 名(45%)实现并保持了至少 10 秒钟的独立坐立(即 ITT 组 32 名患者中有 14 名加上一名用药 181 天的患者)。基线时不需要通气或喂养支持的患者实现坐立的频率更高,这与 STR1VE-US 研究相似。 此外,三名患者在世界卫生组织正常发育窗口期(3-8-9-2 个月19)内实现了独立坐立;四名患者也在世界卫生组织正常发育窗口期内实现了 Bayley-III 独立坐立里程碑。 我们的研究结果表明,虽然服用onasemnogene abeparvovec的无症状脊髓性肌萎缩症1型患者的运动里程碑发育可能会延迟,但5,13,14 独立坐起是可以实现的。 与不需要营养和呼吸支持的患者相比,体征较重、治疗时需要营养或呼吸支持的患者在获得翻身或头部控制等里程碑的年龄较晚。更长的随访期将有助于了解 18 个月后是否能达到更多的里程碑,如坐。
Patients in STR1VE-EU had rapid and sustained improvements in CHOP INTEND scores and scored higher on the Bayley-III gross motor and fine motor subtests. The maximum CHOP INTEND scores for patients in this study were lower than for those in STR1VE-US, which might be because more patients in STR1VE-EU had advanced disease (including lower CHOP INTEND scores) at baseline. Despite these differences, the extent of improvements from baseline and rates at which they were observed were similar. Additionally, infants requiring ventilatory or nutritional support, or both, at baseline showed improvement in motor assessment scores (not observed in the natural history cohort), but improvement was lower than in patients who did not require support at baseline. STR1VE-EU患者的CHOP INTEND评分得到了快速而持续的改善,在Bayley-III粗大运动和精细运动分测验中得分更高。 本研究中患者的 CHOP INTEND 最高分低于 STR1VE-US 中的患者,这可能是因为 STR1VE-EU 中更多患者在基线时已是晚期(包括 CHOP INTEND 分数较低)。 尽管存在这些差异,但与基线相比的改善程度和改善速度是相似的。此外,基线时需要通气或营养支持或同时需要通气和营养支持的婴儿的运动评估评分有所改善(自然病史队列中未观察到),但改善程度低于基线时不需要支持的患者。
In the natural history cohort, 100% of patients older than 12 months required nutritional or combined nutritional and ventilatory support,2 compared with 87% of patients in the STR1VE-EU ability to thrive population who were free from mechanical feeding support at age 18 months. Nearly half of patients who required feeding support at baseline did not require support at the end of the study. Furthermore, a few patients showed the ability to thrive at age 18 months. Notably, bulbar function (eg, swallowing and independence from ventilation and feeding support) was maintained in most patients during the study, which was not seen in natural history data. 在自然病史队列中,12 个月以上的患者 100% 需要营养支持或营养与通气联合支持2,而在 STR1VE-EU 生长能力人群中,87% 的患者在 18 个月时无需机械喂养支持。在基线时需要喂养支持的患者中,近一半在研究结束时不需要喂养支持。此外,少数患者在 18 个月大时表现出茁壮成长的能力。 值得注意的是,大多数患者的球部功能(如吞咽、不需要通气和喂养支持)在研究过程中得以维持,而这在自然病史数据中并不常见。
Nearly all patients (97%) had at least one treatment- emergent adverse event, but few were serious and related to onasemnogene abeparvovec. The most frequently reported drug-related adverse events are included in the product labelling of onasemnogene abeparvovec. Elevations in hepatic aminotransferases were observed in most patients; however, more than 60% of patients had baseline elevations in liver function tests. Although the clinical relevance of this finding remains unclear because the elevations were mild, possible hepatic implications of underlying spinal muscular atrophy have been suggested. Notably, hepatotoxicity was not observed in a long-term follow-up analysis of patients in the START study. Transient isolated reduction in platelets resolved without intervention and did not have clinical implications. Although adverse events of thrombocytopenia were reported in five patients, only one was associated with a decrease in platelets. Importantly, none of the patients had thrombotic microangiopathy and liver failure, which had been reported in some patients who received onasemnogene abeparvovec outside of clinical trials. Due diligence was applied in comprehensive cardiac evaluations and no clinically relevant events were reported. One death occurred in the study, with autopsy data confirming that the cause of death was hypoxic-ischemic brain damage due to a respiratory tract infection because of spinal muscular atrophy type 1, and was considered unrelated to onasemnogene abeparvovec. No new safety signals were identified. 几乎所有患者(97%)都至少出现过一次治疗突发不良事件,但与onasemnogene abeparvovec有关的严重不良事件很少。 最常报告的药物相关不良事件包括在onasemnogene abeparvovec的产品标签中。大多数患者的肝脏转氨酶升高;然而,超过60%的患者肝功能检测基线升高。虽然这一结果的临床意义尚不明确,因为升高的程度较轻,但有人认为潜在的脊髓性肌肉萎缩可能对肝脏有影响。值得注意的是,在对 START 研究中的患者进行长期随访分析时,并未观察到肝毒性。一过性孤立血小板减少无需干预即可缓解,不会产生临床影响。 虽然有五名患者出现血小板减少的不良反应,但只有一人与血小板减少有关。重要的是,没有一名患者出现血栓性微血管病和肝功能衰竭,而在临床试验之外,一些接受onasemnogene abeparvovec治疗的患者曾出现过这种情况。研究人员尽职尽责地进行了全面的心脏评估,未报告任何临床相关事件。研究中发生了一起死亡病例,尸检数据证实死因是1型脊髓性肌萎缩症导致的呼吸道感染引起的缺氧缺血性脑损伤,被认为与onasemnogene abeparvovec无关。 未发现新的安全信号。
Some limitations of interpretation of our safety data mainly surround the use of prednisolone. Although there was protocol specified prednisolone guidance, investi- gators could use clinical discretion in terms of dosing and duration. Variability occurred in the dosing and duration of prednisolone, preventing the ability to make any definitive conclusions. Additionally, the study was limited by its comparison to historical controls. Although this comparison is limited by differences in age at baseline, age at symptom onset, and baseline feeding support requirements, the improvements observed in patients who received onasemnogene abeparvovec have not been previously reported in infants with spinal muscular atrophy type 1, irrespective of age or onset and severity of symptoms. 我们对安全性数据的解释存在一些局限性,主要与泼尼松龙的使用有关。虽然有方案规定的泼尼松龙指导,但在剂量和持续时间方面,研究人员可以使用临床自由裁量权。泼尼松龙的剂量和持续时间存在差异,因此无法得出明确的结论。此外,该研究还受到与历史对照组比较的限制。虽然这种比较受到基线年龄、症状发作年龄和基线喂养支持需求差异的限制,但在接受onasemnogene abeparvovec治疗的患者身上观察到的改善,是以前从未在1型脊髓性肌萎缩症婴儿身上报道过的,无论其年龄或症状发作和严重程度如何。
STR1VE-EU showed the efficacy of onasemnogene abeparvovec, with greater variability in efficacy response than in STR1VE-US because of differences in patient clinical status at baseline. Some of these patients had early onset and more severe disease at enrolment than did patients in STR1VE-US, but showed a response to treatment not only in terms of survival but also in functional aspects. The types of safety events observed were consistent with those described previously. As such, the overall risk–benefit profile for onasemnogene abeparvovec remains favourable for patients with spinal muscular atrophy type 1. STR1VE-EU显示了onasemnogene abeparvovec的疗效,但与STR1VE-US相比,由于患者基线临床状态的差异,疗效反应的变异性更大。 与 STR1VE-US 的患者相比,其中一些患者在入组时发病较早、病情较重,但对治疗的反应不仅体现在存活率方面,还体现在功能方面。观察到的安全事件类型与之前描述的一致。因此,对于1型脊髓性肌萎缩症患者来说,onasemnogene abeparvovec的总体风险-效益分析仍然是有利的。
https://blog.sciencenet.cn/blog-3426442-1434975.html
上一篇:[转载]Onasemnogene abeparvovec基因疗法治疗症状性婴儿型脊髓性肌萎缩症1型-part1